65 7.1 Overview of Alzheimer’s Disease
Learning Objectives
- Understand what Alzheimer’s disease is and its underlying biology.
- Understand different stages of Alzheimer’s disease and its relevant symptoms.
- Learn about the prevalence in the population and its economic impacts.
- Learn about the current treatment for AD and its limitations
What is Alzheimer’s Disease (AD)?

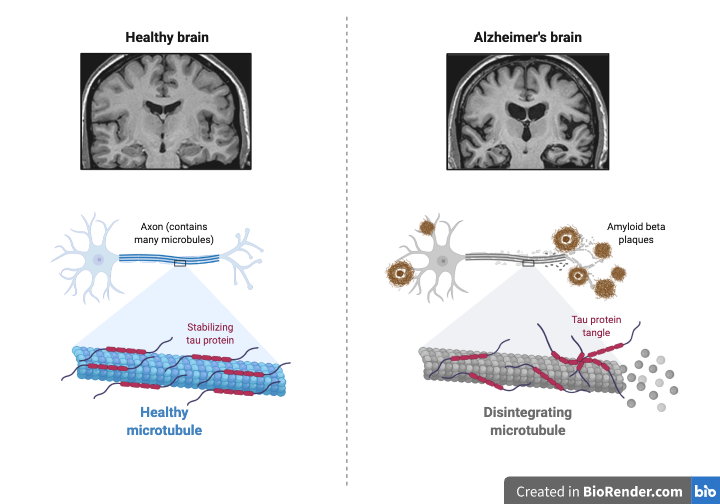
Alzheimer’s Disease (AD) is a neurodegenerative disease that causes dementia among elderly populations with a high prevalence. It is a progressive brain disorder characterizing extracellular accumulation of amyloid β (Aβ) that causes excessive inflammation in the brain (Fang, 2019) (Figure 8.1.1). It is called “progressive” as a definite therapeutic approach to treat AD is not sufficiently developed. Therefore, current therapies aim to slow down the progression of the disease rather than result in a full recovery.
Despite the high prevalence of AD in elderly populations, the exact causes for the disease have not been fully identified. It was reported that about 70% of genetic factors contribute to the expression of AD symptoms, and those that have been exposed to head injuries, depression, and hypertension have a higher risk of developing the disease (Wikipedia).
Previous studies have suggested the potential underlying biology of AD is due to the accumulation of neuroinflammation within the brain (Fang, 2019). This is caused by the interactions between amyloid β (Aβ) and inflammatory receptors, such as TNFR and IL-1R, ultimately leading to memory loss and cognitive impairment as such receptors facilitate learning and memory formation.
Stages of AD

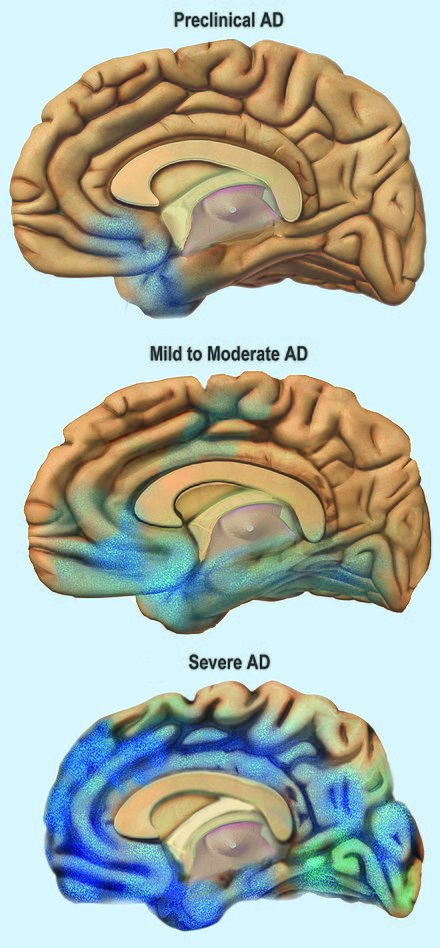
The progressive stages of Alzheimer’s disease are divided into 4 stages: mild cognitive impairment (MCI), early, middle, and late. The initial phase of AD includes mild amnesia that is often misunderstood as a part of the ageing process. Other accompanying symptoms, such as apathy and depression, distinguish AD from ageing or stress. In the early stage, patients with AD start developing speech disorders alongside intensified shortness of memories. They also find themselves having difficulties in learning and accepting new knowledge. The gradual decline in cognition, memory, and linguistic ability accelerates disease progression, which further shifts to the middle stage of AD. Patients with the middle stage start seeking medical assistance for daily living as they lack the ability to perform verbal and non-verbal communications. As AD progresses, the motor ability becomes impaired, making it difficult to carry out daily activities, and the progression of the disorder alters one’s personality to be more irritable. Long-term memory starts to be affected, and patients undergo difficulties in remembering family member’s names. During the most worsened stage of AD, called the late stage, patients become completely dependent on caregivers, and deteriorated symptoms ultimately lead patients to lose their linguistic skills and mobility.
How many Canadians have Alzheimer’s disease?
Approximately 47.5 million people worldwide are reported to suffer from Alzheimer’s disease, and researchers expect the current prevalence of AD to double every 20 years until 2040 (Mayeux and Stern 1). According to a fact report published by Alzheimer’s Association in 2019, approximately 55 million US residents were diagnosed with AD, and this figure is expected to reach 88 million in 30 years. Canada is not an exception to the high prevalence of AD. About 7.1% of Canadian elderly population live with AD (Public Health Agency of Canada). It was reported that women aged over 65 years old are more susceptible to AD, accounting for 65% of the entire patient population (Alzheimer Society of Canada).
Ageing society and AD

Rapid technological advancement in the medical field has provided various clinical insights to measure disease progression via the development of biomarkers and aided in developing a therapeutic approach to treat and further prevent diseases. Consequently, mean life expectancy has significantly improved. According to the World Health Organization (WHO), global healthy life expectancy (HALE) has increased by 8% in 16 years, and the most recently reported global life expectancy in 2016 was 63 years on average. However, prolonged life technology shifts the current society into an ageing society, which has become one of the problematic, yet, unsolved societal issues.
Alzheimer’s disease is one of the most expensive medical conditions in the United States with the costs accumulating to approximately 305 billion dollars in 2020 (Wong, 2020). Although Medicare and Medicaid programs were imposed to reduce financial burdens for seniors receiving medical treatment, one-third of the total cost are still expensed out-of-pocket. The reported average annual expenses for treating AD patients by Medicare and Medicaid in 2019 were $10,814 and $6,234, respectively, while patients without AD had an average cost of $5,953 and $1,962, respectively (Wong, 2020). Consequently, the financial impacts of Alzheimer’s disease have raised the urgency to develop effective treatments. A specific research paper that addresses a potential therapeutic approach for AD will be introduced in the next chapter.
Current Treatment of AD

Current FDA-approved treatments for relieving symptoms of AD are donepezil and memantine. Donepezil also known as Aricept is a cholinesterase inhibitor that is known to treat amnesia among AD patients. It increases acetylcholine availability in the synapse by binding to acetylcholinesterase and inhibiting hydrolysis of acetylcholine in the brain. Since AD has been linked to acetylcholine deficiency in the brain, a cholinesterase inhibitor was introduced to alleviate the amnesia.
Memantine is another FDA-approved medication for treating AD. It is an N-methyl-D-aspartate receptor (NMDAR) antagonist that reduces neuroinflammation by regulating glutamate levels. NMDA receptors belong to the family of ionotropic glutamate receptors and mediate most of the excitatory synaptic transmission in the brain. Previous research suggests that excessive accumulation of amyloid β causes an abnormal increase in extrasynaptic glutamate levels by inhibiting glutamate uptake.
Despite the destructive symptoms and high prevalence of AD, current medications are palliative rather than curative, and new medicines for treating AD have not been developed or approved by the FDA since 2003. Developing AD therapies has become a great interest in the global community, and the field of dementia and Alzheimer’s disease is one of the most prominently studied research fields.
Chapter Summary
Alzheimer’s Disease (AD) is a neurodegenerative disease that causes dementia among 60% of elderly populations with a high prevalence. It is a progressive brain disorder that gets worsened over time, characterizing extracellular accumulation of amyloid β (Aβ) that causes excessive inflammation in the brain. An estimated 47.5 million populations worldwide and 7% of the elderly Canadians were reported to suffer from AD. The onset of AD is characterized by 4 stages: mild cognitive impairment (MCI), early, middle and late or advanced stage. Amnesia is the initial determinant of AD, and patients start developing deficits in linguistic ability, motor ability, and cognition as it gets worsened over time. Despite the high prevalence of AD in elderly populations, current FDA-approved treatments for relieving symptoms are donepezil and memantine. Donepezil and memantine are used to alleviate amnesia and neuroinflammation, however, they do not have the efficacy to treat AD fully. Due to the high prevalence and destructive symptoms of AD, the importance of AD therapy development is greatly emphasized in the global community.
References
“What Is Alzheimer’s Disease?” National Institute on Aging, U.S. Department of Health and Human Services, www.nia.nih.gov/health/what-alzheimers-disease.
“What Is Alzheimer’s?” Alzheimer’s Disease and Dementia, Alzheimer’s Association , www.alz.org/alzheimers-dementia/what-is-alzheimers.
Mayeux, Richard, and Yaakov Stern. “Epidemiology of Alzheimer Disease.” Cold Spring Harbor Perspectives in Medicine, Cold Spring Harbor Laboratory Press, 1 Aug. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3405821/.
“Alzheimer’s Disease.” Wikipedia, Wikimedia Foundation, 30 Nov. 2020, en.wikipedia.org/wiki/Alzheimer’s_disease.
Canada, Public Health Agency of. “Government of Canada.” Dementia in Canada, Including Alzheimer’s Disease: Highlights from the Canadian Chronic Disease Surveillance System – Canada.ca, / Gouvernement Du Canada, 21 Sept. 2017, www.canada.ca/en/public-health/services/publications/diseases-conditions/dementia-highlights-canadian-chronic-disease-surveillance.html.
Wong, Winston. “Economic Burden of Alzheimer Disease and Managed Care Considerations.” AJMC, 17 Aug. 2020, www.ajmc.com/view/economic-burden-of-alzheimer-disease-and-managed-care-considerations.
“World Health Statistics 2020 Visual Summary.” World Health Organization, www.who.int/data/gho/whs-2020-visual-summary. Accessed 13 Dec. 2020.
Kumar, Anil. “Donepezil.” StatPearls [Internet]., U.S. National Library of Medicine, 22 Aug. 2020, www.ncbi.nlm.nih.gov/books/NBK513257/.
Derivative form of Amyloid Precursor Protein (APP)
National health insurance in the United States
National health care system aims to reduce financial burdens for low-income US citizens