5.7 Other Ventilation Modes
As previously mentioned, the basic modes of ventilation are volume and pressure. All other modes are derivatives of the basic modes. Many of these modes use a closed loop feedback algorithm where the ventilator has the ability to interpret data measured from the patients and make adjustments to target certain parameters.
Pressure Regulated Volume Control Ventilation (PRVC)
PRVC can be described as a mode in which breaths are patient or time triggered, pressure regulated, volume targeted, and time cycled. In this mode, the clinician establishes a target tidal volume based on the patient's ideal body weight. The ventilator will start ventilation with a volume controlled breath during which it measures lung compliance and the pressure required to inflate the lung. For subsequent breaths, the ventilator then measures the delivered tidal volume and compares it to the set target. If there is a discrepancy, the ventilator automatically adjusts the pressure to achieve the desired volume. You may find this mode with different names on different ventilators. In clinical setting, ensure that you familiarize yourself with each ventilator and available modes. PRVC is also known as: Adaptive Pressure Ventilation (APV) Volume Control + (VC+).
To ensure patient safety, it is crucial to set an appropriate upper pressure limit when using PRVC. Most ventilators have safeguards in place to prevent pressure adjustments from exceeding [latex]5\text{ cmH}_2\text{O}[/latex] below the defined upper pressure limit.
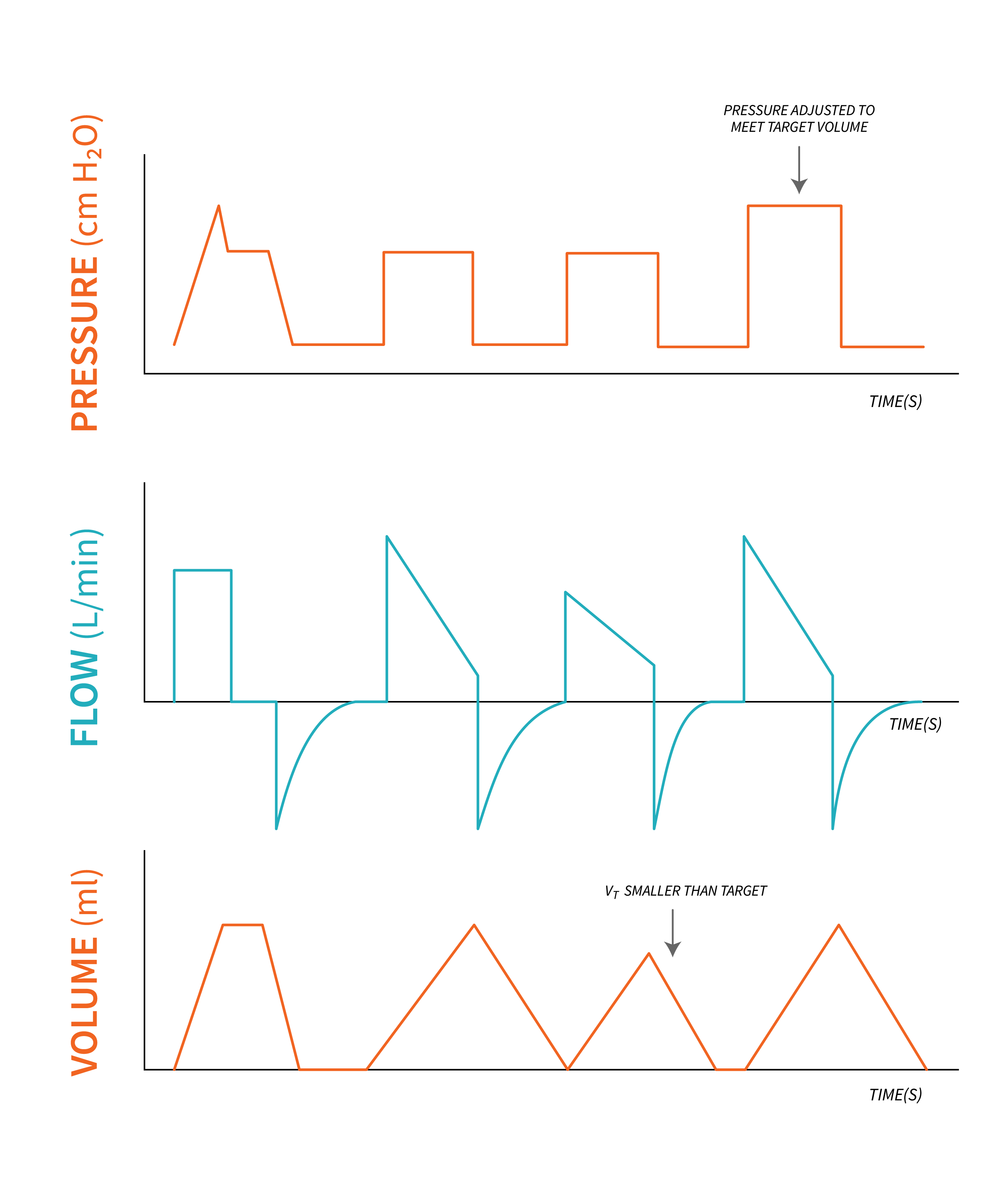
PRVC has been described as an adaptive targeting mode in which the ventilator uses a feedback mechanism on a breath-by-breath basis to dynamically regulate the delivered pressure and achieve the desired tidal volume target. PRVC attempts to combine the advantages of variable flow from pressure control mode with the guaranteed minute ventilation of VC volume control mode.
|
Summary of Basic Settings in PRVC |
|
|---|---|
In PRVC, you will directly set:
|
In PRVC, the ventilator will set/ determine:
|
For more information on PRVC, watch this video:
Adaptive Support Ventilation (ASV)
The Adaptive Support Ventilation (ASV) mode allows the clinician to set a target minute volume based on the patient's ideal body weight.
Minute volume, IBW, sex (the ventilator uses this information to determine IBW range), FiO2, PEEP, Maximum pressure limit. Normal Minute volume is on average, [latex]10\text{ mL/Kg}[/latex] IBW. With this information from the clinician, the ventilator then determines the minimum respiratory rate and tidal volume required to meet the target minute volume and deliver the necessary pressure or breaths to achieve that.
|
Summary of Basic Settings in ASV |
|
|---|---|
In ASV, you will directly set:
|
In ASV, the ventilator will set:
|
ASV combines and alternates a control mode with pressure with a spontaneous mode with pressure based on the patient's level of consciousness and ability to trigger and maintain breaths to ensure minimal work of breathing is required from the patient.
Mandatory Minute Ventilation (MMV)
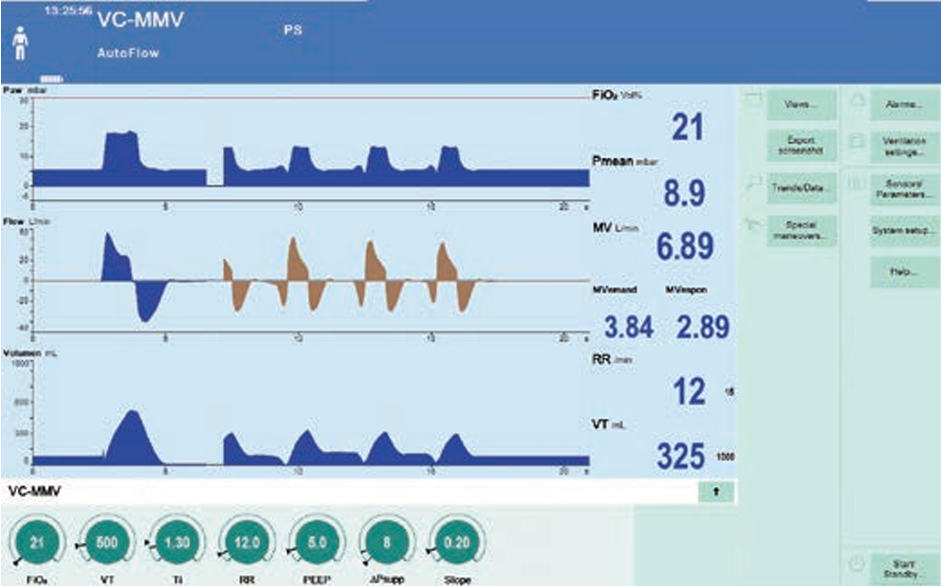
Mandatory Minute Ventilation (MMV) is another example of a closed loop feedback ventilation mode intended to guarantee minimum minute ventilation in which the ventilator recognizes patient effort and contributes with whatever part the patient is unable to maintain, either the respiratory rate or tidal volume. It combines spontaneous breaths initiated by the patient and supported with pressure by the ventilator with volume controlled mandatory breaths.
Mandatory breaths are provided by the ventilator when spontaneous breaths are insufficient and fall below the set minute volume. As spontaneous breathing increases, fewer mandatory breaths are provided. With this ventilation mode, the patient always receives at least the set minimum minute volume (Remember, [latex]V_E=V_T\times RR[/latex]). In this mode, pressure and flow are adjusted so that tidal volume is reached with the minimum necessary pressure for the volume controlled breaths based on changes in lung mechanics (compliance and resistance).
Below is a screenshot from a Draeger ventilator showing MMV with volume control and Autoflow feature (Figure 5.7.2).
Automode
Automode is available on some ventilators such as the Servo I and Servo U, this ventilation mode introduces an interactive strategy, where the ventilator can switch between pressure control and pressure support, as well as volume control and volume support, based on the patient's needs.
When the patient's respiratory drive decreases and/or mechanics indicate the need for full ventilation with pressure control, the ventilator will deliver breaths in pressure control mode providing a set pressure with each breath. This helps ensure consistent and controlled ventilation when needed, while allowing the patient to breathe spontaneously when they are able. Conversely, when the patient's respiratory mechanics allow for volume control, the ventilator will operate in volume control mode, delivering a set tidal volume with adjusted pressure support. The ability of AutoMode to switch between pressure control and pressure support, as well as volume control and volume support, allows for adaptive respiratory support based on the patient's lung characteristics and changing respiratory needs.
Note: there are other ventilation modes used in clinical practice often classified as Advanced Ventilation Modes, such as Bilevel Ventilation, Airway Pressure Release Ventilation (APRV), High Frequency Oscillation ventilation (HFOV). We will discuss these modes in more detail in a later chapters.
