5.1 Using Control Modes of Ventilation
When mechanical ventilation is indicated, it is normally because the patients are not oxygenating or ventilating appropriately. Indications for mechanical ventilation include: hypoxic failure, hypercapnia (or respiratory failure) and ineffective drive to breathe. When patients are acutely ill and experiencing indications for ventilation, their body cannot effectively balance their oxygenation or CO2 clearance needs without intervention. They are intubated and ventilated to take over control of these imbalances. A control mode of ventilation is the obvious choice, as there is a need to fully take over how much and how often the patient is breathing, since they are ineffective in fixing it on their own.
Key Takeaway
When patients experience conditions such as hypoxia, hypercapnia, or a compromised drive to breathe, their breathing needs to be supported, and a control mode is utilized to address the underlying ventilation issue. It’s important to note that while mechanical ventilation does not cure the underlying illnesses causing respiratory problems, it serves to supplement patient effort and reduce respiratory muscle workload, enabling the body to allocate more energy towards the healing and repair processes.
We have already discussed that there are two categories of control modes. One that is described via the volume of air delivered and one described by the pressure applied to the lungs. Let’s narrow our focus to the control mode branch of the ventilation “family tree:”
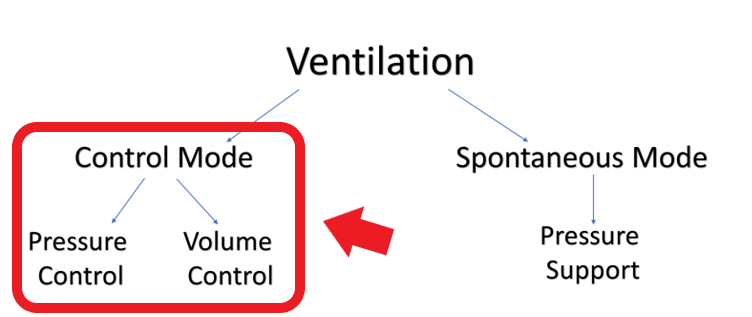
So you have identified the need to control ventilate your patient, but now we have a choice to make: do we use pressure control or volume control? Which one is better?
We previously discussed that both of these modes describe the exact same thing—air being pushed into the lungs. Realistically, once you understand the premise of these modes, you would be able to ventilate essentially the same in pressure or in volume by manipulating all of the settings on the ventilator. Though described in different ways, they are two sides of the same coin. Whether it be pressure or volume, both control modes are simply a set amount of air being pushed in at a set rate.
Key Takeaway
Take a look at the following acronyms which are commonly used by clinicians when talking about volume or pressure control:
- [latex]\textbf{A/C}=\text{assist/control (used to refer to control mode in general)}[/latex]
- [latex]\textbf{PC}\text{ or }\textbf{PCV}=\text{pressure control or pressure control ventilation}[/latex]
- [latex]\textbf{VC}\text{ or }\textbf{VCV}=\text{volume control or volume control ventilation}[/latex]
This might look a bit like “alphabet soup” to you, but don’t be anxious. Just translate these short-forms to control mode, pressure control or volume control, and you will understand perfectly. Over time, you will become more familiar with these acronyms and begin to use them yourself.
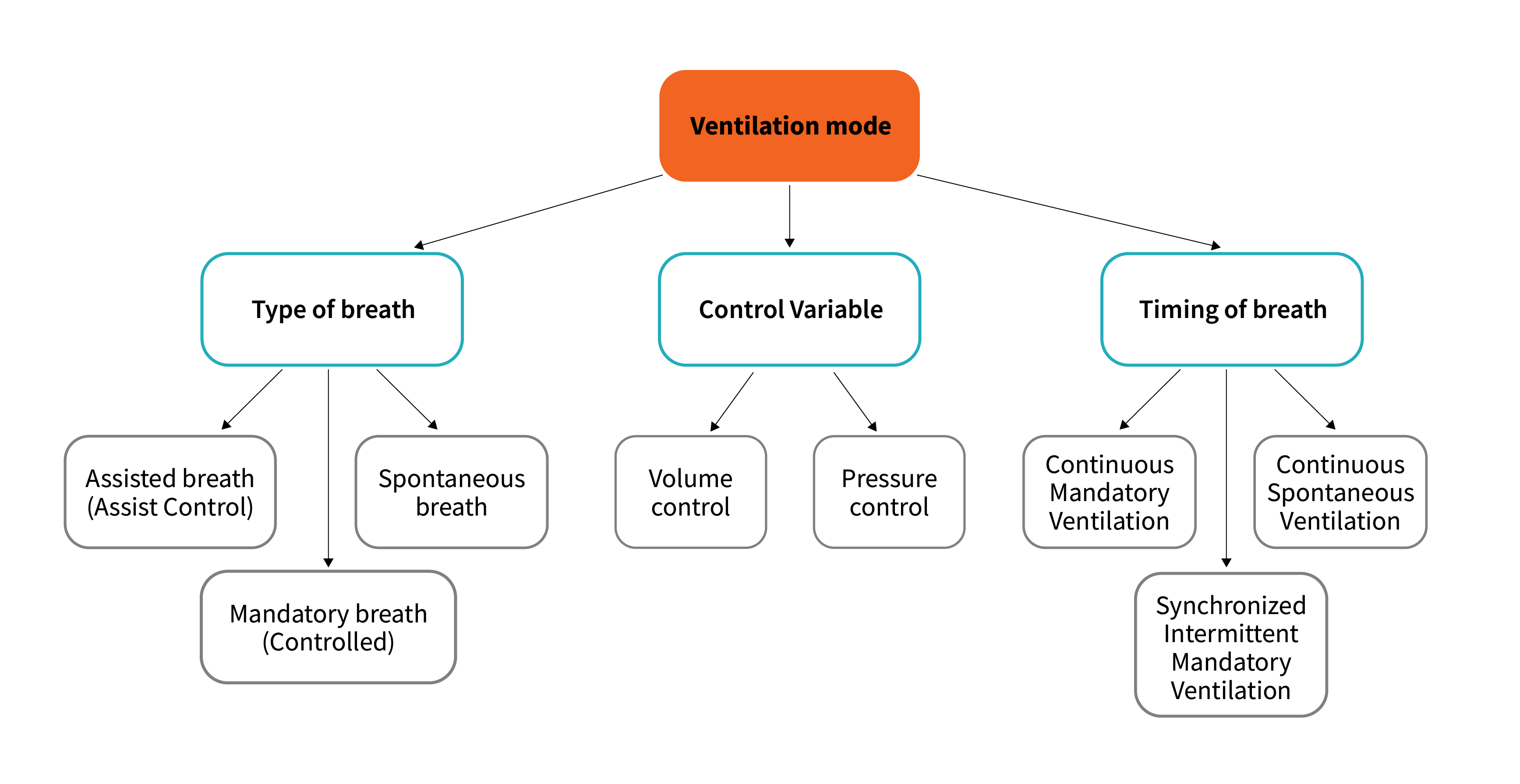
We have now gained enough knowledge about breath control and delivery to be able to define a ventilation mode based on the type of breath delivered, the control variable for each breath and the timing of breaths. The specific phase variable (trigger, limit, cycle, baseline) depends on the mode selected.
With controlled ventilation, all breaths are mandatory (controlled), meaning they are delivered independent of patient effort and are time triggered.
Example
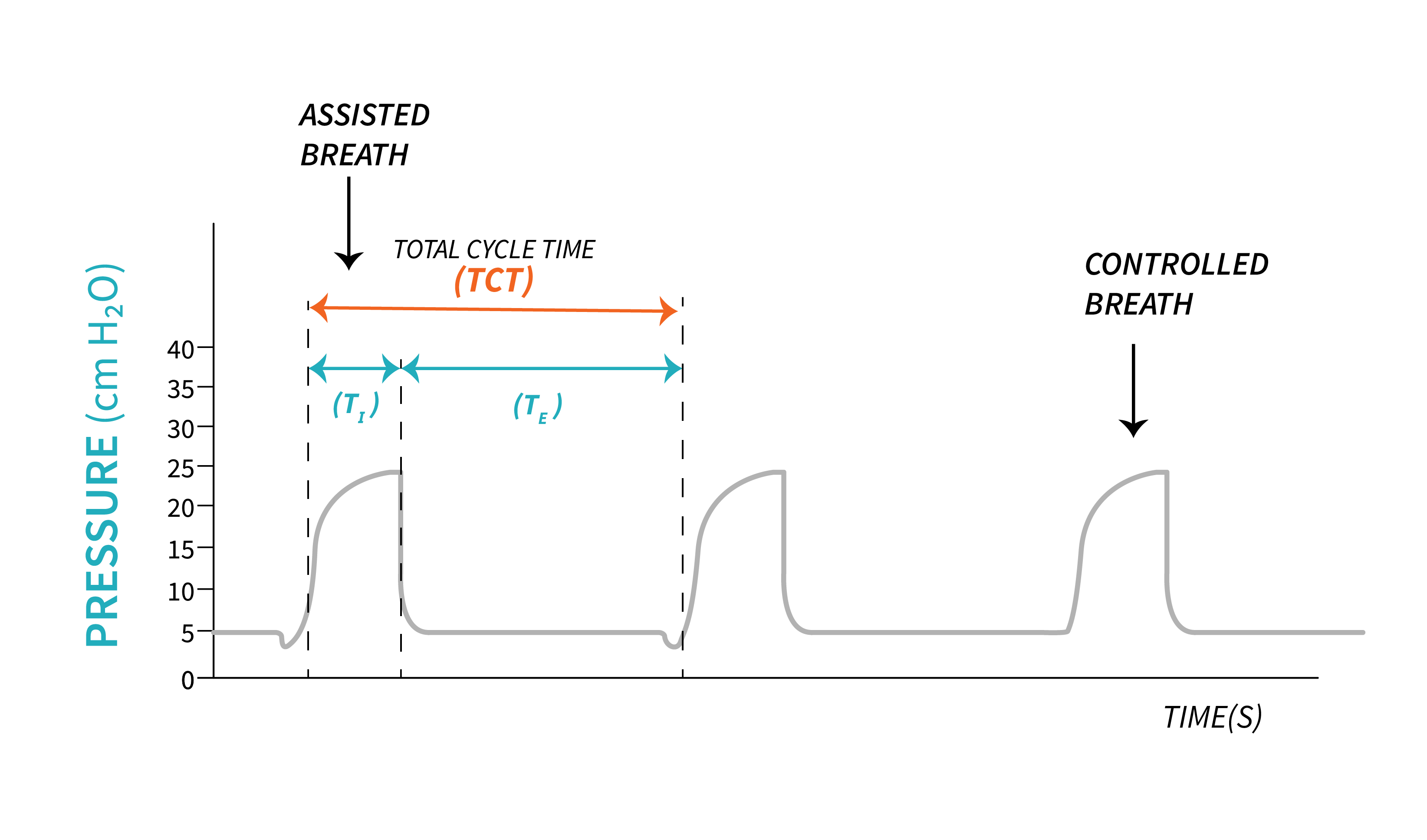
Fully controlled ventilation mode is mostly a thing of the past as most ventilators today provide Continuous Mandatory Ventilation (CMV) also known as Assist Control Ventilation. With Assist Control (A/C) ventilation, breaths can be time triggered or patient-triggered. This mode is sensitive to patient effort, allowing patient triggering based on the sensitivity set by the clinician. The limit and cycle variable depend on the control variable used (volume, flow, pressure). The assist control mode offers an advantage by ensuring a minimum rate, which proves beneficial when patients are unable to initiate respiratory efforts. Simultaneously, it allows patients to trigger breaths beyond the minimum set rate according to their individual needs. When patients initiate a breath, the ventilator detects the trigger and delivers a mandatory breath based on the limits, cycle, and baseline set by the clinician. Consequently, in assist control ventilation, all breaths (both time-triggered and patient-triggered) exhibit uniform characteristics including the same limits, cycle, and baseline, with the trigger variable being the only distinguishing factor.
Example
RT set a rate of 12. The patient will receive a breath every 5 seconds.
If patient requirements increase, and they start triggering the ventilator above the set rate of 12.
The ventilator will recognize those triggers, and deliver as many breaths as the patient requires. All breaths will have the same limit, cycle and baseline (all breaths will look the same)
Intermittent Mandatory Ventilation (IMV) is another ventilation strategy determined by the timing of breaths delivery. Breaths are delivered at present time intervals. This is a type of partially supportive mode as it allows patients to take spontaneous breaths in between mandatory breaths. This feature is different than Assist Control ventilation where the patient may trigger a breaths but the ventilator takes over and delivers a mandatory breath. When the patient triggers a breath during IMV, in between mandatory breaths, that breath will be spontaneous and can be supported or unsupported (more on this when we discuss spontaneous ventilation modes). Because there is no synchronization between ventilator delivered breath and patient’s own spontaneous breaths, this mode may lead to breaths stacking when a mandatory breath is delivered on top of a spontaneous breath or the patient takes a spontaneous breath on top of a mandatory breath.
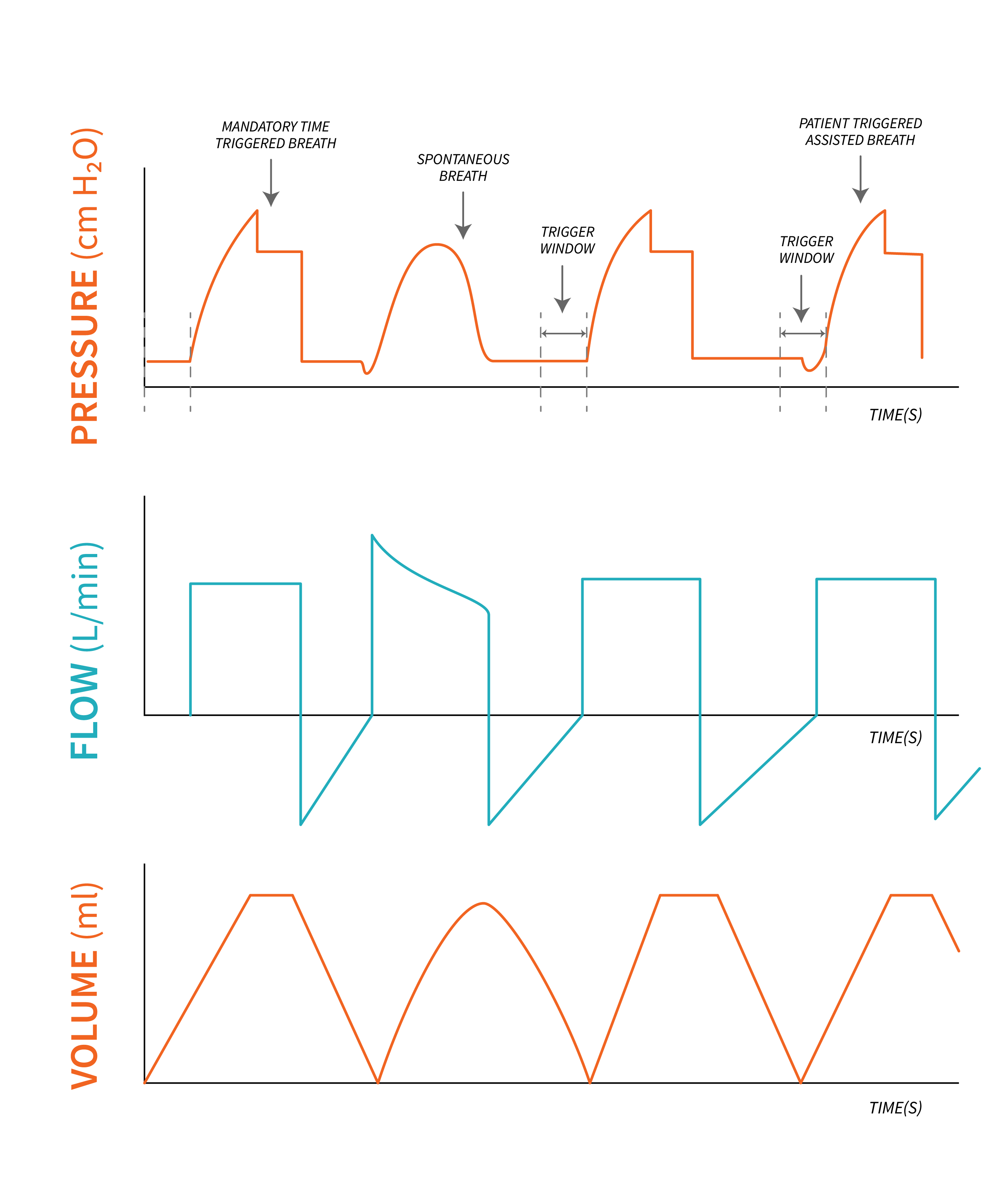
Most ventilators today are capable of synchronization and offer Synchronized Intermittent Mandatory Ventilation (SIMV). There is still a set rate in this mode, but the patient can dictate their own respiratory rate, as they can take spontaneous breaths in between mandatory breaths. This mode allows three different types of breaths: mandatory, assisted and spontaneous breaths. An assisted breath is delivered in SIMV, when the patient triggers the ventilator (makes an inspiratory effort) during the trigger window. This so called window represents a short period of time, just before a mandatory breath is delivered, based on preset time, when the ventilator becomes sensitive to any inspiratory effort (trigger), and will deliver an assisted breath. This is similar to the assist control mode described above. However, if the patient makes an inspiratory effort outside of the trigger window, then the patient will receive a spontaneous breath. If patient makes no effort in that trigger window then the ventilator will initiate a time triggered mandatory breath.
Key Takeaway
The trigger window can be likened to a key that unlocks the door to a breath. Just like a key activates the mechanism to open a door, the trigger in SIMV initiates the delivery of a assisted breath. It allows the patient to have control over when they need assistance with their breathing. Once the trigger has sensed by the ventilator, it responds by providing an assisted breath, ensuring that the patient’s respiratory needs are met. Similar to how a key triggers the unlocking process, the trigger window in SIMV acts as a gateway, enabling synchronized and coordinated ventilation for the patient’s comfort.
 |
 |
Example
With a set rate in SIMV of [latex]10\text{ bpm}[/latex]—the ventilator delivers [latex]1\text{ breath}[/latex] every [latex]6\text{ seconds}[/latex].
If the trigger window is [latex]0.5\text{ seconds}[/latex], then at [latex]5.5\text{ seconds}[/latex] from the onset of the last mandatory breath the ventilator becomes sensitive to any spontaneous effort, and will deliver an assisted breath. In the absence of a spontaneous effort, the ventilator delivers a time triggered, mandatory breath.
SIMV can be a challenge to understand, as it is usually a combination of control, assisted and spontaneous breaths. This mode is not used to a large degree in most Intensive Care Units due to large amounts of research that have identified inherent issues in asynchrony and increased length of ICU stays. With more adaptive modes available today, this ventilation mode is losing popularity. However, you may still encounter it, and use it in certain patients for weaning purposes where variable amounts of work of breathing are required.
“Using Control Modes of Ventilation” from Basic Principles of Mechanical Ventilation by Melody Bishop, © Sault College is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.

{kind=link}
{kind=link}