21 Sexuality in Young Adulthood

Human sexuality refers to people’s sexual interest in and attraction to others, as well as their capacity to have erotic experiences and responses. Sexuality may be experienced and expressed in a variety of ways, including thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. These may manifest themselves in biological, physical, emotional, social, or spiritual aspects. The biological and physical aspects of sexuality largely concern the human reproductive functions, including the human sexual-response cycle and the basic biological drive that exists in all species. Emotional aspects of sexuality include bonds between individuals that are expressed through profound feelings or physical manifestations of love, trust, and care. Social aspects deal with the effects of human society on one’s sexuality, while spirituality concerns an individual’s spiritual connection with others through sexuality. Sexuality also impacts, and is impacted by cultural, political, legal, philosophical, moral, ethical, and religious aspects of life.
The Sexual Response Cycle
Sexual motivation, often referred to as libido, is a person’s overall sexual drive or desire for sexual activity. This motivation is determined by biological, psychological, and social factors. In most mammalian species, sex hormones control the ability to engage in sexual behaviors. However, sex hormones do not directly regulate the ability to copulate in primates (including humans); rather, they are only one influence on the motivation to engage in sexual behaviors. Social factors, such as work and family also have an impact, as do internal psychological factors like personality and stress. Sex drive may also be affected by hormones, medical conditions, medications, lifestyle stress, pregnancy, and relationship issues.
The sexual response cycle is a model that describes the physiological responses that take place during sexual activity. According to Kinsey, Pomeroy, and Martin (1948), the cycle consists of four phases: excitement, plateau, orgasm, and resolution. The excitement phase is the phase in which the intrinsic (inner) motivation to pursue sex arises. The plateau phase is the period of sexual excitement with increased heart rate and circulation that sets the stage for orgasm. Orgasm is the release of tension, and the resolution period is the unaroused state before the cycle begins again.
The Brain and Sex
The brain is the structure that translates the nerve impulses from the skin into pleasurable sensations. It controls nerves and muscles used during sexual behavior. The brain regulates the release of hormones, which are believed to be the physiological origin of sexual desire. The cerebral cortex, which is the outer layer of the brain that allows for thinking and reasoning, is believed to be the origin of sexual thoughts and fantasies. Beneath the cortex is the limbic system, which consists of the amygdala, hippocampus, cingulate gyrus, and septal area. These structures are where emotions and feelings are believed to originate, and are important for sexual behavior.
The hypothalamus is the most important part of the brain for sexual functioning. This is the small area at the base of the brain consisting of several groups of nerve-cell bodies that receives input from the limbic system. Studies with lab animals have shown that destruction of certain areas of the hypothalamus causes complete elimination of sexual behavior. One of the reasons for the importance of the hypothalamus is that it controls the pituitary gland, which secretes hormones that control the other glands of the body.
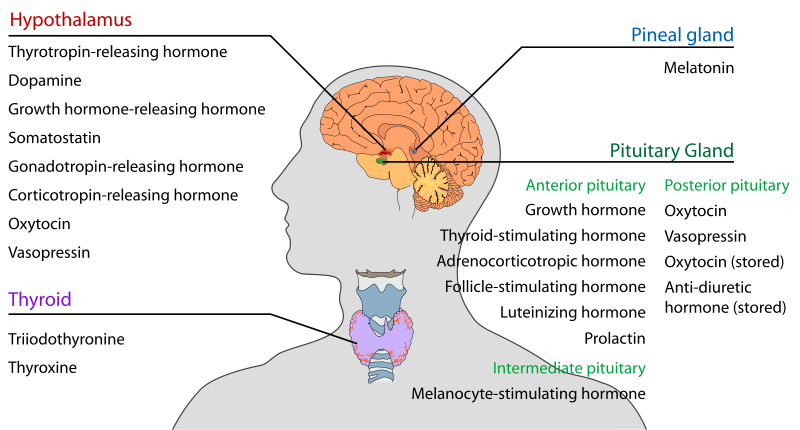
Hormones
Several important sexual hormones are secreted by the pituitary gland. Oxytocin, also known as the hormone of love, is released during sexual intercourse when an orgasm is achieved. Oxytocin is also released in females when they give birth or are breast feeding; it is believed that oxytocin is involved with maintaining close relationships. Both prolactin and oxytocin stimulate milk production in females. Follicle-stimulating hormone (FSH) is responsible for ovulation in females by triggering egg maturity; it also stimulates sperm production in males. Luteinizing hormone (LH) triggers the release of a mature egg in females during the process of ovulation.
In males, testosterone appears to be a major contributing factor to sexual motivation. Vasopressin is involved in the male arousal phase, and the increase of vasopressin during erectile response may be directly associated with increased motivation to engage in sexual behavior.
The relationship between hormones and female sexual motivation is not as well understood, largely due to the overemphasis on male sexuality in Western research. Estrogen and progesterone typically regulate motivation to engage in sexual behavior for females, with estrogen increasing motivation and progesterone decreasing it. The levels of these hormones rise and fall throughout a woman’s menstrual cycle. Research suggests that testosterone, oxytocin, and vasopressin are also implicated in female sexual motivation in similar ways as they are in males, but more research is needed to understand these relationships.
Sexual Responsiveness Peak
Men and women tend to reach their peak of sexual responsiveness at different ages. For men, sexual responsiveness tends to peak in the late teens and early twenties. Sexual arousal can easily occur in response to physical stimulation or fantasizing. Sexual responsiveness begins a slow decline in the late twenties and into the thirties, although a man may continue to be sexually active. Through time, a man may require more intense stimulation in order to become aroused. Women often find that they become more sexually responsive throughout their 20s and 30s and may peak in the late 30s or early 40s. This is likely due to greater self-confidence and reduced inhibitions about sexuality.
Sexually Transmitted Infections
Sexually transmitted infections (STIs), also referred to as sexually transmitted diseases (STDs) or venereal diseases (VDs), are illnesses that have a significant probability of transmission by means of sexual behavior, including vaginal intercourse, anal sex, and oral sex. Some STIs can also be contracted by sharing intravenous drug needles with an infected person, as well as through childbirth or breastfeeding.
Common STIs include:
- chlamydia
- herpes (HSV-1 and HSV-2)
- human papillomavirus (HPV)
- gonorrhea
- syphilis
- trichomoniasis
- HIV (human immunodeficiency virus) and AIDS (acquired immunodeficiency syndrome)
According to the Centers for Disease Control and Prevention (CDC) (2014), there was an increase in the three most common types of STDs in 2014. These include 1.4 million cases of chlamydia, 350,000 cases of gonorrhea, and 20,000 cases of syphilis. Those most affected by STDS include those younger, gay/bisexual males, and females. The most effective way to prevent transmission of STIs is to practice safe sex and avoid direct contact of skin or fluids which can lead to transfer with an infected partner. Proper use of safe-sex supplies (such as male condoms, female condoms, gloves, or dental dams) reduces contact and risk and can be effective in limiting exposure; however, some disease transmission may occur even with these barriers.
Material in this chapter up to here taken directly from Lally & Valentine-French (2017). The following two paragraphs were written by Baird. Photographs in the remaining part of this chapter were gathered by O’Neil, McCarthy, & Williams.
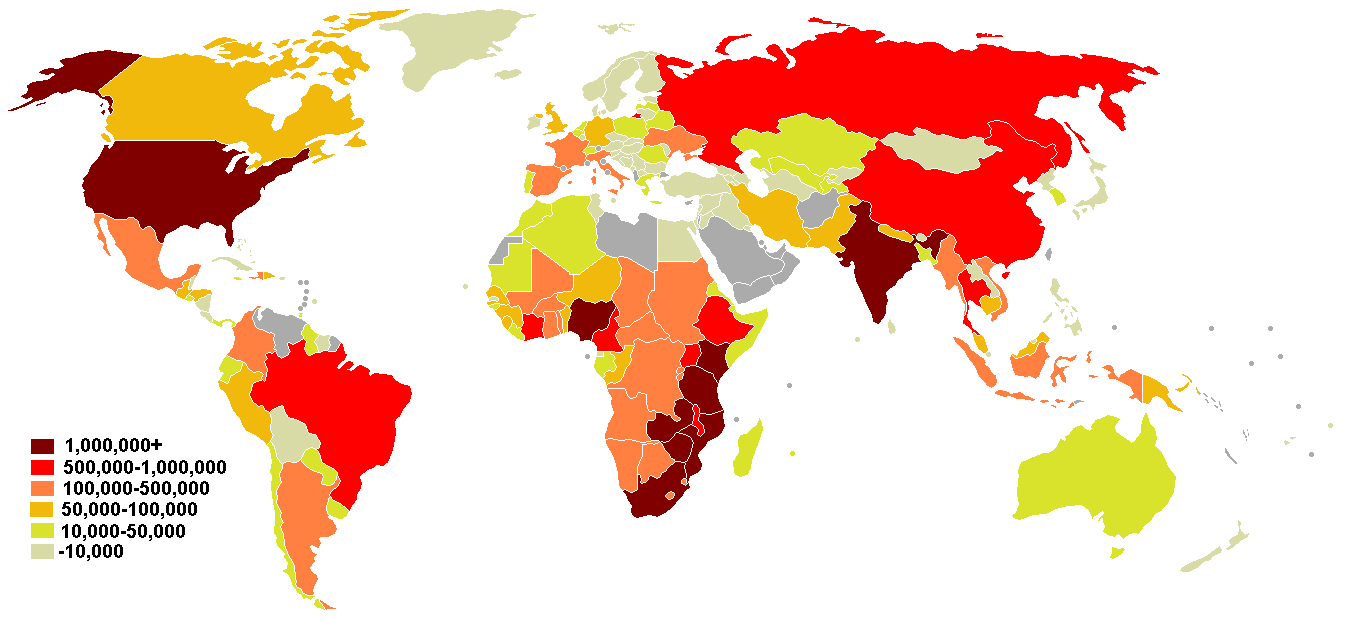
The same three STIs are the most common in Canada. A CBC News (2019) article noted that chlamydia and gonorrhea rates across Canada soared in Canada in 2017, the last year for which statistics were available. Although the nation-wide rate of syphilis infection dipped slightly in 2017, it had risen steeply over the past 10 years (178%) with increases of 49% and 81% for gonorrhea.
These increases and concerns also apply worldwide according to the World Health Organization (WHO, 2019, especially to populations with low SES, sex workers, men who have sex with women. There is particular concern about under-utilization of condoms, especially female condoms, and increasing problems with antibiotic-resistant strains of gonorrhea. Untreated STIs can cause lifelong severe problems, such as infertility. In other words, the rise in STIs is a cohort-specific adult development concern. Prevention and treatment methods for STIs are topics adults should follow actively throughout their lifespan.
Societal Views on Sexuality
Society’s views on sexuality are influenced by everything from religion to philosophy, and they have changed throughout history and are continuously evolving. Historically, religion has been the greatest influence on sexual behavior in the United States; however, in more recent years, peers and the media have emerged as two of the strongest influences, particularly among American teens (Potard, Courtois, & Rusch, 2008).
Mass media in the form of television, magazines, movies, and music continues to shape what is deemed appropriate or normal sexuality, targeting everything from body image to products meant to enhance sex appeal. Media serves to perpetuate a number of social scripts about sexual relationships and the sexual roles of men and women, many of which have been shown to have both empowering and problematic effects on people’s (especially women’s) developing sexual identities and sexual attitudes.
Cultural Differences
In the West, premarital sex is normative by the late teens, more than a decade before most people enter marriage. In the United States and Canada, and in northern and eastern Europe, cohabitation is also normative; most people have at least one cohabiting partnership before marriage. In southern Europe, cohabiting is still taboo, but premarital sex is tolerated in emerging adulthood. In contrast, both premarital sex and cohabitation remain rare and forbidden throughout Asia. Even dating is discouraged until the late twenties, when it would be a prelude to a serious relationship leading to marriage. In cross-cultural comparisons, about three fourths of emerging adults in the United States and Europe report having had premarital sexual relations by age 20, versus less than one fifth in Japan and South Korea (Hatfield & Rapson, 2006).
Sexual Orientation
A person’s sexual orientation is their emotional and sexual attraction to a particular sex or gender. It is a personal quality that inclines people to feel romantic or sexual attraction (or a combination of these) to persons of a given sex or gender. According to the American Psychological Association (APA) (2016), sexual orientation also refers to a person’s sense of identity based on those attractions, related behaviors, and membership in a community of others who share those attractions.
Sexual Orientation on a Continuum

Sexuality researcher Alfred Kinsey was among the first to conceptualize sexuality as a continuum rather than a strict dichotomy of gay or straight. To classify this continuum of heterosexuality and homosexuality, Kinsey et al. (1948) created a seven-point rating scale that ranged from exclusively heterosexual to exclusively homosexual. Research done over several decades has supported this idea that sexual orientation ranges along a continuum, from exclusive attraction to the opposite sex/gender to exclusive attraction to the same sex/gender (Carroll, 2016).

However, sexual orientation now can be defined in many ways. Heterosexuality, which is often referred to as being straight, is attraction to individuals of the opposite sex/gender, while homosexuality, being gay or lesbian, is attraction to individuals of one’s own sex/gender. Bisexuality was a term traditionally used to refer to attraction to individuals of either male or female sex, but it has recently been used in nonbinary models of sex and gender (i.e., models that do not assume there are only two sexes or two genders) to refer to attraction to any sex or gender. Alternative terms such as pansexuality and polysexuality have also been developed, referring to attraction to all sexes/genders and attraction to multiple sexes/genders, respectively (Carroll, 2016).
Asexuality refers to having no sexual attraction to any sex/gender. According to Bogaert (2015) about one percent of the population is asexual. Being asexual is not due to any physical problems, and the lack of interest in sex does not cause the individual any distress. Asexuality is being researched as a distinct sexual orientation.
Development of Sexual Orientation
According to current scientific understanding, individuals are usually aware of their sexual orientation between middle childhood and early adolescence. However, this is not always the case, and some do not become aware of their sexual orientation until much later in life. It is not necessary to participate in sexual activity to be aware of these emotional, romantic, and physical attractions; people can be celibate and still recognize their sexual orientation. Some researchers argue that sexual orientation is not static and inborn, but is instead fluid and changeable throughout the lifespan.
There is no scientific consensus regarding the exact reasons why an individual holds a particular sexual orientation. Research has examined possible biological, developmental, social, and cultural influences on sexual orientation, but there has been no evidence that links sexual orientation to one factor (APA, 2016). Biological explanations, that include genetics, hormones, and birth order, will be explored further.
Using both twin and familial studies, heredity provides one biological explanation for sexual orientation. Bailey and Pillard (1991) studied pairs of male twins and found that the concordance rate for identical twins was 52%, while the rate for fraternal twins was only 22%. Bailey, Pillard, Neale, and Agyei (1993) studied female twins and found a similar difference with a concordance rate of 48% for identical twins and 16% for fraternal twins. Schwartz, Kim, Kolundzija, Rieger, and Sanders (2010) found that gay men had more homosexual male relatives than heterosexual men, and sisters of gay men were more likely to be lesbians than sisters of straight men.
Excess or deficient exposure to hormones during prenatal development has also been theorized as an explanation for sexual orientation. One-third of females exposed to abnormal amounts of prenatal androgens, a condition called congenital adrenal hyperplasia (CAH), identify as bisexual or lesbian (Cohen-Bendahan, van de Beek, & Berenbaum, 2005). In contrast, too little exposure to prenatal androgens may affect male sexual orientation by not masculinizing the male brain (Carlson, 2011).
Another explanation attempts to explain why gay men tend to have a greater number of older brothers than heterosexual men (Blanchard, 2001). This difference is explained by the maternal immune hypothesis which proposes “a progressive immunization to male-specific antigens after the birth of successive sons in some mothers, which increases the effect of anti-male antibodies on the sexual differentiation of the brain in the developing fetus” (Carroll, 2016, p. 264). Consequently, in some families with multiple brothers, those born later have demonstrated higher rates of homosexuality.
Sexual Orientation Discrimination
The United States is heteronormative, meaning that society supports heterosexuality as the norm. Consider, for example, that homosexuals are often asked, “When did you know you were gay?” but heterosexuals are rarely asked, “When did you know you were straight?” (Ryle, 2011). Living in a culture that privileges heterosexuality has a significant impact on the ways in which non-heterosexual people are able to develop and express their sexuality.
Open identification of one’s sexual orientation may be hindered by homophobia which encompasses a range of negative attitudes and feelings toward homosexuality or people who are identified or perceived as being lesbian, gay, bisexual, or transgender (LGBT). It can be expressed as antipathy, contempt, prejudice, aversion, or hatred; it may be based on irrational fear and is sometimes related to religious beliefs (Carroll, 2016). Homophobia is observable in critical and hostile behavior, such as discrimination and violence on the basis of sexual orientations that are non- heterosexual. Recognized types of homophobia include institutionalized homophobia, such as religious and state-sponsored homophobia, and internalized homophobia in which people with same-sex attractions internalize, or believe, society’s negative views and/or hatred of themselves.

Gay men, lesbians, and bisexual people regularly experience stigma, harassment, discrimination, and violence based on their sexual orientation (Carroll, 2016). Research has shown that gay, lesbian, and bisexual teenagers are at a higher risk of depression and suicide due to exclusion from social groups, rejection from peers and family, and negative media portrayals of homosexuals (Bauermeister et al., 2010). Discrimination can occur in the workplace, in housing, at schools, and in numerous public settings. Much of this discrimination is based on stereotypes and misinformation. Major policies to prevent discrimination based on sexual orientation have only come into effect in the United States in the last few years.
The majority of empirical and clinical research on lesbian, gay, bisexual, and transgender (LGBT) populations are done with largely white, middle-class, well-educated samples. This demographic limits our understanding of more marginalized sub-populations that are also affected by racism, classism, and other forms of oppression. In the United States, non-Caucasian LGBT individuals may find themselves in a double minority, in which they are not fully accepted or understood by Caucasian LGBT communities, and are also not accepted by their own ethnic group (Tye, 2006). Many people experience racism in the dominant LGBT community where racial stereotypes merge with gender stereotypes.
The Canadian Mental Health Association website notes that discrimination against sexual and gender minorities is widespread in Canada, especially for transgender individuals, and especially for those of more than one marginalized group (Canadian Mental Health Association and Rainbow Health Ontario, 2019). However, the website posts a list of research-backed measures that societies and individuals can take to reduce or eliminate the harmful effects of discrimination.
Except for the paragraph above and change in the term gay to the preferred gay men, text in this chapter is taken directly from Lally & Valentine-French (2017). Photographs were collected by O’Neil, McCarthy, & Williams. Glossary definitions generally are quoted directly from the APA
Dictionary of Psychology (undated).
Media Attributions
- 039-couplehands
- 042-BrainSex © UNAIDS 2008 Global Report is licensed under a CC BY-SA (Attribution ShareAlike) license
- 043-GayMen © Marcelo Chagas is licensed under a CC0 (Creative Commons Zero) license
- 043-LesbianCouple © Felipe Balduino is licensed under a CC0 (Creative Commons Zero) license
- 043-StopHomophobia © EYE DJ is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
1. the capacity to derive pleasure from various forms of sexual activity and behavior, particularly from sexual intercourse.
2. all aspects of sexual behavior, including gender identity, orientation, attitudes, and activity. (quoted directly from APA Dictionary of Psychology, undated)
1. in psychoanalytic theory, either the psychic energy of the life instinct in general or the energy of the sexual instinct in particular. In his first formulation, Sigmund Freud conceived of this energy as narrowly sexual, but subsequently he broadened the concept to include all expressions of love, pleasure, and self-preservation. See also Eros.
2. in the analytic psychology of Carl Jung, the general life force that provides energy for all types of activities: biological, sexual, social, cultural, and creative.
3. more generally, sexual energy or desire.
a conceptualization of a four-stage cycle of sexual response exhibited by both men and women, differing only in aspects determined by male or female anatomy. The stages include the arousal (or excitement) phase, which lasts several minutes to hours (see sexual arousal); the plateau phase, lasting 30 seconds to 3 minutes, marked by penile erection in men and vaginal lubrication in women; the orgasmic phase, lasting 15 seconds and marked by ejaculation in men and orgasm in women; and the resolution phase, lasting 15 minutes to 1 day (see refractory phase). This conceptualization was introduced by U.S. sex researchers William H. Masters (1915–2001) and Virginia E. Johnson (1925–2013) in 1966, but it has subsequently been criticized, particularly in the way that it equates the male and female pattern.
the part of the brain that helps integrate autonomic activity into appropriate responses to internal and external stimuli - involved in appetite, thirst, sleep, and sexuality.
a peptide produced in the hypothalamus and released by the posterior pituitary gland into the blood, where it acts as a hormone, or into the central nervous system, where it acts as a neurotransmitter and binds to oxytocin receptors to influence behavior and physiology.
It has earned a reputation as a facilitator of social affiliation, and the tend-and-befriend response in particular, and it has been shown to influence sexual pleasure, reproductive functions, and parental (especially material) behaviour.
a gonadotropin released by the anterior pituitary gland that, in females, stimulates the development in the ovary of graafian follicles (see menstrual cycle). The same hormone in males stimulates Sertoli cells in the testis to produce spermatozoa.
a gonadotropin secreted by the anterior pituitary gland that, in females, stimulates the rapid growth of a graafian follicle in the ovary until it ruptures and releases an ovum (see menstrual cycle). In males, it stimulates the interstitial cells of the testis to secrete androgens.
a peptide produced in the hypothalamus and released by the posterior pituitary gland into the blood as controlled by osmoreceptors. Additionally, vasopressin and the chemically related peptide hormone oxytocin have been implicated in a range of mammalian social behaviors, such as aggression, territoriality, maternal and paternal care, pair-bond formation and mating, social recognition, attachment, affiliation, and vocalization, as well as components of human-specific social behaviors and disorders (e.g., autism).
any of a class of steroid hormones that are produced mainly by the ovaries and act as the principal female sex hormones, inducing estrus in female mammals and secondary female sexual characteristics in humans. [...] Estrogens are used therapeutically in estrogen replacement therapy and oral contraceptives and to treat certain menstrual disorders and some types of breast and prostate cancers.
a hormone, secreted mainly by the corpus luteum in the ovary, that stimulates the proliferation of the endometrium (lining) of the uterus required for implantation of an embryo. If implantation occurs, progesterone continues to be secreted—first by the corpus luteum and then by the placenta—maintaining the pregnant uterus and preventing further release of egg cells from the ovary. It also stimulates development of milk-secreting cells in the breasts.
an infection transmitted by sexual activity. More than 20 STIs have been identified, including those caused by viruses (e.g., hepatitis B, herpes, HIV) and those caused by bacteria (e.g., chlamydia, gonorrhea, syphilis).
one's enduring sexual attraction to male, female, and other-gendered partners. Sexual attraction may be hetersexual, same sex (gay or lesbian), bisexual, pansexual, asexual (no sexual attraction), or any number of other identified labels.
sexual attraction to or activity between members of the opposite sex
sexual attraction or activity between members of the same sex. Although the term can refer to homosexual orientation in both men and women, current practice distinguishes between gay men and lesbians, and homosexuality itself is now commonly referred to as same-sex sexual orientation or activity.
sexual attraction to or sexual behavior with both men and women. Although much psychological research demonstrates the existence of a continuum of sexual attraction within most individuals, equal responsiveness to both sexes over the lifespan is relatively rare, appearing to be more common in women than in men and varying across cultures.
not limited in sexual choice with regard to biological sex, gender, or gender identity
sexual attraction to more than one gender
lacking sexual drive or sexual attraction to others; asexual people may still experience attraction, but it does not need to manifest itself in a sexual manner
the assumption that heterosexuality is the standard for defining normal sexual behavior and that male–female differences and gender roles are the natural and immutable essentials in normal human relations. According to some social theorists, this assumption is fundamentally embedded in, and legitimizes, social and legal institutions that devalue, marginalize, and discriminate against people who deviate from its normative principle (e.g., gay men, lesbians, bisexuals, transgendered persons).
dread or fear of gay men and lesbians, associated with prejudice and anger toward them, that leads to discrimination in such areas as employment, housing, and legal rights and sometimes to violence (gay bashing). Extreme homophobia may lead to murder.

{kind=link}