33 Psychosocial Development in Middle Adulthood
There are many socioemotional changes that occur in how middle-aged adults perceive themselves. While people in their early 20s may emphasize how old they are to gain respect or to be viewed as experienced, by the time people reach their 40s they tend to emphasize how young they are. For instance, few 40 year olds cut each other down for being so young stating: “You’re only 43? I’m 48!” A previous focus on the future gives way to an emphasis on the present. Neugarten (1968) notes that in midlife, people no longer think of their lives in terms of how long they have lived. Rather, life is thought of in terms of how many years are left.
Midlife Crisis?
Although the hoopla about the midlife crisis usually is attributed to Daniel Levinson, who was a U.S. psychologist, an Atlantic article (Druckerman, 2018) makes the case that the phenomenon was first reported in modern history by a Canadian physician and psychoanalyst, Elliott Jaques, who reported that people commonly had a depressive experience in their mid-30s that lasted several years.
In 1978 Daniel Levinson published a book entitled The Seasons of a Man’s Life in which he presented a theory of development in adulthood. Levinson’s work was based on in-depth interviews with 40 men between the ages of 35-45. Levinson (1978) indicated that adults go through stages and have an image of the future that motivates them. This image is called “the dream” and for the men interviewed, it was a dream of how their career paths would progress and where they would be at midlife. According to Levinson the midlife transition (40-45) was a time of reevaluating previous commitments; making dramatic changes if necessary; giving expression to previously ignored talents or aspirations; and feeling more of a sense of urgency about life and its meaning. By the time the men entered middle adulthood (45-50), they believed they committed to the new choices made and placed one’s energies into these commitments.
Levinson believed that a midlife crisis was a normal part of development as the person is more aware of how much time has gone by and how much time is left. The future focus of early adulthood gives way to an emphasis on the present in midlife, and the men interviewed had difficulty reconciling the “dream” they held about the future with the reality they experienced. Consequently, they felt impatient and were no longer willing to postpone the things they had always wanted to do. Although Levinson believed his research demonstrated the existence of a midlife crisis, his study has been criticized for his research methods, including small sample size, similar ages, and concerns about a cohort effect. In fact, other research does not support his theory of the midlife crisis.
Vaillant (2012) believed that it was the cross-sectional design of Levinson’s study that led to the erroneous conclusion of an inevitable midlife crisis. Instead, he believed that longitudinal studies of an individual’s entire life was needed to determine the factors associated with optimum health and potential. Vaillant was one of the main researchers in the 75 year-old Harvard Study of Adult Development, and he considered a midlife crisis to be a rare occurrence among the participants (Vaillant, 1977). Additional findings of this longitudinal study will be discussed in the next chapter on late adulthood.
Most research suggests that most people in the United States today do not experience a midlife crisis. Results of a 10-year study conducted by the MacArthur Foundation Research Network on Successful Midlife Development, based on telephone interviews with over 3,000 midlife adults, suggest that the years between 40 and 60 are ones marked by a sense of well-being. Only 23% of their participants reported experiencing a midlife crisis. The crisis tended to occur among the highly educated and was triggered by a major life event rather than out of a fear of aging (Research Network on Successful Midlife Development, 2007).
Stress

We all know that stress plays a major role in our mental and physical health, but what exactly is stress? The term stress is defined as a pattern of physical and psychological responses in an organism after it perceives a threatening event that disturbs its homeostasis and taxes its abilities to cope with the event (Hooker & Pressman, 2016). Stress was originally derived from the field of mechanics where it is used to describe materials under pressure. The word was first used in a psychological manner by researcher Hans Selye, who was examining the effect of an ovarian hormone that he thought caused sickness in a sample of rats. Surprisingly, he noticed that almost any injected hormone produced this same sickness. He smartly realized that it was not the hormone under investigation that was causing these problems, but instead the aversive experience of being handled and injected by researchers led to high physiological arousal, and eventually to health problems like ulcers.
Selye (1946) coined the term stressor to label a stimulus that had this effect on the body (that is, causing stress). He developed a model of the stress response called the General Adaptation Syndrome, which is a three-phase model of stress, which includes a mobilization of physiological resources phase, a coping phase, and an exhaustion phase (i.e., when an organism fails to cope with the stress adequately and depletes its resources). Image 5.33.2 illustrates the General Adaptation Syndrome.

Psychologists have studied stress in a myriad of ways, and it is not just major life stressor (e.g., a family death, a natural disaster) that increase the likelihood of getting sick. Stress can result from negative events, chronically difficult situations, a biological fight-or-flight response, and as clinical illness, such as post-traumatic stress disorder (PTSD). Even small daily hassles, like getting stuck in traffic or fighting with your friend, can raise your blood pressure, alter your stress hormones, and even suppress your immune system function (DeLongis, Folkman, & Lazarus, 1988; Twisk, Snel, Kemper, & van Machelen, 1999). Stress continues to be one of the most important and well-studied psychological correlates of illness, because excessive stress causes potentially damaging wear and tear on the body and can influence almost any disease process.
Dispositions and Stress
Negative dispositions and personality traits have been strongly tied to an array of health risks. One of the earliest negative trait-to-health connections was discovered in the 1950s by two cardiologists. They made the interesting discovery that there were common behavioral and psychological patterns among their heart patients that were not present in other patient samples. This pattern included being competitive, impatient, hostile, and time urgent. They labeled it Type A Behavior. Importantly, it was found to be associated with double the risk of heart disease as compared with Type B Behavior (absence of Type A behaviors) (Friedman & Rosenman, 1959). Since the 1950s, researchers have discovered that it is the hostility and competitiveness components of Type A that are especially harmful to heart health (Iribarren et al., 2000; Matthews, Glass, Rosenman, & Bortner, 1977; Miller, Smith, Turner, Guijarro, & Hallet, 1996). Hostile individuals are quick to get upset, and this angry arousal can damage the arteries of the heart. In addition, given their negative personality style, hostile people often lack a heath-protective supportive social network.
Social Relationships and Stress

Research has shown that the impact of social isolation on our risk for disease and death is similar in magnitude to the risk associated with smoking regularly (Holt-Lunstad, Smith, & Layton, 2010; House, Landis, & Umberson, 1988). In fact, the importance of social relationships for our health is so significant that some scientists believe our body has developed a physiological system that encourages us to seek out our relationships, especially in times of stress (Taylor et al., 2000). Social integration is the concept used to describe the number of social roles that you have (Cohen & Willis, 1985). For example, you might be a daughter, a basketball team member, a Humane Society volunteer, a coworker, and a student. Maintaining these different roles can improve your health via encouragement from those around you to maintain a healthy lifestyle. Those in your social network might also provide you with social support (e.g., when you are under stress). This support might include emotional help (e.g., a hug when you need it), tangible help (e.g., lending you money), or advice. By helping to improve health behaviors and reduce stress, social relationships can have a powerful, protective impact on health, and in some cases, might even help people with serious illnesses stay alive longer (Spiegel, Kraemer, Bloom, & Gottheil, 1989).
Caregiving and Stress
A disabled child, spouse, parent, or other family member is part of the lives of some midlife adults. According to the National Alliance for Caregiving (2015), 40 million Americans provide unpaid caregiving. The typical caregiver is a 49 year-old female currently caring for a 69 year-old female who needs care because of a long-term physical condition. Looking more closely at the age of the recipient of caregiving, the typical caregiver for those 18-49 years of age is a female (61%) caring mostly for her own child (32%) followed by a spouse or partner (17%). When looking at older recipients (50+) who receive care, the typical caregiver is female (60%) caring for a parent (47%) or spouse (10%).
Caregiving places enormous stress on the caregiver. Caregiving for a young or adult child with special needs was associated with poorer global health and more physical symptoms among both fathers and mothers (Seltzer, Floyd, Song, Greenberg, & Hong, 2011). Marital relationships are also a factor in how the caring affects stress and chronic conditions. Fathers who were caregivers identified more chronic health conditions than non-caregiving fathers, regardless of marital quality. In contrast, caregiving mothers reported higher levels of chronic conditions when they reported a high level of marital strain (Kang & Marks, 2014). Age can also make a difference in how one is affected by the stress of caring for a child with special needs. Using data from the Study of Midlife in the Unites States, Ha, Hong, Seltzer and Greenberg (2008) found that older parents were significantly less likely to experience the negative effects of having a disabled child than younger parents. They concluded that an age-related weakening of the stress occurred over time. This follows with the greater emotional stability noted at midlife.
Currently 25% of adult children, mainly baby boomers, provide personal or financial care to a parent (Metlife, 2011). Daughters are more likely to provide basic care and sons are more likely to provide financial assistance. Adult children 50+ who work and provide care to a parent are more likely to have fair or poor health when compared to those who do not provide care. Some adult children choose to leave the work force, however, the cost of leaving the work force early to care for a parent is high. For females, lost wages and social security benefits equals $324,044, while for men it equals $283,716 (Metlife, 2011). This loss can jeopardize the adult child’s financial future. Consequently, there is a need for greater workplace flexibility for working caregivers.
Spousal Care
Certainly caring for a disabled spouse would be a difficult experience that could negatively affect one’s health. However, research indicates that there can be positive health effect for caring for a disabled spouse. Beach, Schulz, Yee and Jackson (2000) evaluated health related outcomes in four groups: Spouses with no caregiving needed (Group 1), living with a disabled spouse but not providing care (Group 2), living with a disabled spouse and providing care (Group 3), and helping a disabled spouse while reporting caregiver strain, including elevated levels of emotional and physical stress (Group 4). Not surprisingly, the participants in Group 4 were the least healthy and identified poorer perceived health, an increase in health-risk behaviors, and an increase in anxiety and depression symptoms. However, those in Group 3 who provided care for a spouse, but did not identify caregiver strain, actually identified decreased levels of anxiety and depression compared to Group 2 and were actually similar to those in Group 1. It appears that greater caregiving involvement was related to better mental health as long as the caregiving spouse did not feel strain. The beneficial effects of helping identified by the participants were consistent with previous research (Krause, Herzog, & Baker, 1992; Schulz et al., 1997).

When caring for a disabled spouse, gender differences have also been identified. Female caregivers of a spouse with dementia experienced more burden, had poorer mental and physical health, exhibited increased depressive symptomatology, took part in fewer health- promoting activities, and received fewer hours of help than male caregivers (Gibbons et al., 2014). This recent study was consistent with previous research findings that women experience more caregiving burden than men, despite similar caregiving situations (Torti, Gwyther, Reed, Friedman, & Schulman, 2004; Yeager, Hyer, Hobbs, & Coyne, 2010). Explanations for why women do not use more external support, which may alleviate some of the burden, include women’s expectations that they should assume caregiving roles (Torti et al, 2004) and their concerns with the opinions of others (Arai, Sugiura, Miura, Washio, & Kudo, 2000). Also contributing to women’s poorer caregiving outcomes is that disabled males are more aggressive than females, especially males with dementia who display more physical and sexual aggression toward their caregivers (Eastley & Wilcock, 1997; Zuidema, de Jonghe, Verhey, & Koopmans, 2009). Female caregivers are certainly at risk for negative consequences of caregiving, and greater support needs to be available to them.
Stress Management
About 20% of Americans report having stress, with 18–33 year-olds reporting the highest levels (American Psychological Association, 2012). Given that the sources of our stress are often difficult to change (e.g., personal finances, current job), a number of interventions have been designed to help reduce the aversive responses to duress, especially related to health. For example, relaxation activities and forms of meditation are techniques that allow individuals to reduce their stress via breathing exercises, muscle relaxation, and mental imagery. Physiological arousal from stress can also be reduced via biofeedback, a technique where the individual is shown bodily information that is not normally available to them (e.g., heart rate), and then taught strategies to alter this signal. This type of intervention has even shown promise in reducing heart and hypertension risk, as well as other serious conditions (Moravec, 2008; Patel, Marmot, & Terry, 1981). Reducing stress does not have to be complicated. For example, exercise is a great stress reduction activity (Salmon, 2001) that has a myriad of health benefits.
Coping Strategies

Coping is often classified into two categories: problem-focused coping or emotion-focused coping (Carver, Scheier, & Weintraub, 1989). Problem-focused coping is thought of as actively addressing the event that is causing stress in an effort to solve the issue at hand. For example, say you have an important exam coming up next week. A problem-focused strategy might be to spend additional time over the weekend studying to make sure you understand all of the material. Emotion-focused coping, on the other hand, regulates the emotions that come with stress. In the above examination example, this might mean watching a funny movie to take your mind off the anxiety you are feeling. In the short term, emotion-focused coping might reduce feelings of stress, but problem-focused coping seems to have the greatest impact on mental wellness (Billings & Moos, 1981; Herman-Stabl, Stemmler, & Petersen, 1995). That being said, when events are uncontrollable (e.g., the death of a loved one), emotion-focused coping directed at managing your feelings, at first, might be the better strategy. Therefore, it is always important to consider the match of the stressor to the coping strategy when evaluating its plausible benefits.
Erikson: Generativity vs Stagnation
According to Erikson (1982) generativity encompasses procreativity, productivity, and creativity. This stage includes the generation of new beings, new products, and new ideas, as well as self-generation concerned with further identity development. Erikson believed that the stage of generativity, during which one established a family and career, was the longest of all the stages. Individuals at midlife are primarily concerned with leaving a positive legacy of themselves, and according to Erikson (1950) parenthood is the primary generative type. Erikson understood that work and family relationships may be in conflict due to the obligations and responsibilities of each, but he believed it was overall a positive developmental time. In addition to being parents and working, Erikson also described individuals being involved in the community during this stage. A sense of stagnation occurs when one is not active in generative matters, however, stagnation can motive a person to redirect energies into more meaningful activities.
Erikson identified “virtues” for each of his eight stages, and they refer to what the individual achieves when the stage is successfully reconciled. The virtue emerging when one achieves generativity is “Care”. Erikson believed that those in middle adulthood should “take care of the persons, the products, and the ideas one has learned to care for” (Erikson, 1982, p. 67). Further, Erikson believed that the strengths gained from the six earlier stages are essential for the generational task of cultivating strength in the next generation. Erikson further argued that generativity occurred best after the individual had resolved issues of identity and intimacy (Peterson & Duncan, 2007).
Research has demonstrated that generative adults possess many positive characteristics, including good cultural knowledge and healthy adaptation to the world (Peterson & Duncan, 2007). Using the Big 5 personality traits, generative women and men scored high on conscientiousness, extraversion, agreeableness, openness to experience, and low on neuroticism (de St. Aubin & McAdams, 1995; Peterson, Smirles, & Wentworth, 1997). Additionally, women scoring high in generativity at age 52, were rated high in positive personality characteristics, satisfaction with marriage and motherhood, and successful aging at age 62 (Peterson & Duncan, 2007). Similarly, men rated higher in generativity at midlife were associated with stronger global cognitive functioning (e.g., memory, attention, calculation), stronger executive functioning (e.g., response inhibition, abstract thinking, cognitive flexibility), and lower levels of depression in late adulthood (Malone, Liu, Vaillant, Rentz, & Waldinger, 2016).
Erikson (1982) indicated that at the end of this demanding stage, individuals may withdraw as generativity is no longer expected in late adulthood. Erickson thought of this as a release of older people from caring and working. However, as we have seen with other stage theories, research shows that a strict progression stage by stage is not the way we go through life. Instead, a spiral (Malone et al., 2016) may better describe the progression through Erikson’s developmental challenges and achievements. In other words, overall we make progress, but we revisit earlier conflicts, regrets, task, and opportunities, and sometimes come away with renewed strength and new skills. We also must remember that Erikson himself was embedded in the culture of the early 50s and did not know of the increased possibilities for vitality in life that can be possible as societies provide the technological innovations and environments that promote health and contributions for more years.
Seen this way, generativity earlier in life does far more than make it possible for us to feel satisfied with life as we get older. Instead it powers more generativity and contributions right on through life. Societies which facilitate intergenerational contact and opportunities for everyone to participate will be more generative societies with people living longer and more happily. From studies such as research on the Blue Zones we know this can happen: https://www.bluezones.com/
Midlife Relationships
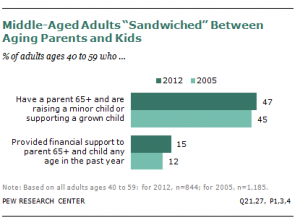
The sandwich generation refers to adults who have at least one parent age 65 or older and are either raising their own children or providing support for their grown children. According to a recent Pew Research survey, 47% of middle-aged adults are part of this sandwich generation (Parker & Patten, 2013). In addition, 15% of middle-aged adults are providing financial support to an older parent while raising or supporting their own children (see Figure 5.33.6). According to the same survey, almost half (48%) of middle-aged adults, have supported their adult children in the past year, and 27% are the primary source of support for their grown children.
Seventy-one percent of the sandwich generation is age 40-59, 19% were younger than 40, and 10% were 60 or older. Hispanics are more likely to find themselves supporting two generations; 31% have parents 65 or older and a dependent child, compared with 24% of whites and 21% of blacks (Parker & Patten, 2013). Women are more likely to take on the role of care provider for older parents in the U.S. and Germany (Pew Research, 2015). About 1 in 5 women say they have helped with personal care, such as getting dressed or bathing, of aging parents in the past year, compared with 8% of men in the U.S. and 4% in Germany. In contrast, in Italy men are just as likely (25%) as women (26%) to have provided personal care.
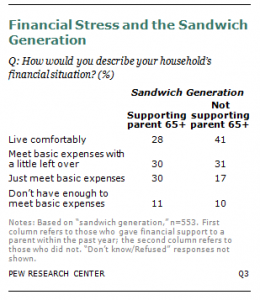
The Pew survey found that almost 1 in 3 of the sandwich-generation adults were more likely to say they always feel rushed, while only 23% of other adults said this. However, the survey suggests that those who were supporting both parents and children reported being just as happy as those middle-aged adults who did not find themselves in the sandwich generation (Parker & Patten, 2013). Adults who are supporting both parents and children did report greater financial strain (see Figure 5.33.7). Only 28% reported that they were living comfortably versus 41% of those who were not also supporting their parents. Almost one third were just making ends meet, compared with 17% of those who did not have the additional financial burden of aging parents.
Kinkeeping
At midlife adults may find themselves as a kinkeeper. In all families there is a person or persons who keep the family connected and who promote solidarity and continuity in the family (Brown & DeRycke, 2010). Who in your own family do you count on to organize family gatherings? Who knows the history of your family? Who do people turn to in your family for advice and support? Who works to strengthen the bonds between members of your family? These are your family’s kinkeepers, and they are usually women (Leach & Braithwaite, 1996; Brown & DeRycke, 2010). Leach and Braithwaite found that 86% of their respondents named a woman as their family’s kinkeeper, and Brown and DeRycke found that mothers, maternal grandmothers, and paternal grandmothers were more likely to be a family’s kinkeeper than were fathers, young adult children, and grandfathers combined. Brown and DeRycke also found that among young adults, women were more likely to be a kinkeeper than were young adult men.
Kinkeeping can be a source of distress when it interferes with other obligations (Gerstel & Gallagher, 1993). Gerstel and Gallagher found that on average, kinkeepers provide almost a full week of work each month to kinkeeping (almost 34 hours). They also found that the more activities the kinkeeper took on, and the more kin they helped the more stress and higher the levels of depression a kinkeeper experienced. However, unlike other studies on kinkeeping, Gerstel and Gallagher also included a number of activities that would be considered more “caregiving,” such as providing transportation, making repairs, providing meals, etc. in addition to the usual activities of kinkeeping.
Empty nest
The empty nest, or post-parental period (Dennerstein, Dudley & Guthrie, 2002), refers to the time period when children are grown up and have left home. For most parents this occurs during midlife. This time is recognized as a “normative event” as parents are aware that their children will become adults and eventually leave home (Mitchell & Lovegreen, 2009). The empty nest creates complex emotions, both positive and negative, for many parents. Some theorists suggest this is a time of role loss for parents, others suggest it is one of role strain relief (Bouchard, 2013).
The role loss hypothesis predicts that when people lose an important role in their life they experience a decrease in emotional well-being. It is from this perspective that the concept of the empty nest syndrome emerged, which refers to great emotional distress experienced by parents, typically mothers, after children have left home. The empty nest syndrome is linked to the absence of alternative roles for the parent in which they could establish their identity (Borland, 1982). In Bouchard’s (2013) review of the research, she found that few parents reported loneliness or a big sense of loss once all their children had left home.
In contrast, the role stress relief hypothesis suggests that the empty nest period should lead to more positive changes for parents, as the responsibility of raising children has been lifted. The role strain relief hypothesis was supported by many studies in Bouchard’s (2013) review. A consistent finding throughout the research literature is that raising children has a negative impact on the quality of martial relationships (Ahlborg, Misvaer, & Möller, 2009; Bouchard, 2013). Several studies have reported that martial satisfaction often increases during the launching phase of the empty nest period, and that this satisfaction endures long after the last child has left home (Gorchoff, John, & Helson, 2008).
However, most of the research on the post-parental period has been with American parents. A number of studies in China suggest that empty-nesters, especially in more rural areas of China, report greater loneliness and depression than their counterparts with children still at home (Wu et al., 2010). Family support for the elderly by their children is a cherished Chinese tradition (Wong & Leung, 2012). With children moving from the rural communities to the larger cities for education and employment this may explain the more pessimistic reaction of Chinese parents than in American samples. The loss of an adult child in a rural region may mean a loss of family income for aging parents. Empty-nesters in urban regions of China did not report the same degree of distress (Su et al., 2012), suggesting that it not so much the event of children leaving, but the additional hardships this may place on aging parents.
Boomerang Kids
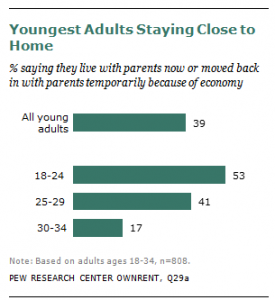
Young adults are living with their parents for a longer duration and in greater numbers than previous generations. In addition to those in early adulthood who are not leaving the home of their parents, there are also young adults who are returning after having lived independently outside the home, and these are called boomerang kids. Figure 5.33.8 shows the number of young people who are still living at home (Parker, 2012). In addition, 63% of 18 to 34 year- olds know someone who has returned to live with their parents. Many of the same financial reasons that are influencing young people’s decisions to delay exit from the home of their parents are underlying their decisions to return home. In addition, to financial reasons, some boomerang kids are returning because of emotional distress, such as mental health issues (Sandberg-Thoma, Snyder, & Jang, 2015).
What is the effect on parents when their adult children return home? Certainly there is considerable research that shows that the stress of raising children can have a negative impact on parents’ well-being, and that when children leave home many couples experience less stress and greater life satisfaction (see the section on the empty nest). Early research in the 1980s and 1990s supported the notion that boomerang children, along with those who were failing to exit the home, placed greater financial hardship on the parents, and the parents reported more negative perceptions of this living arrangement (Aquilino, 1991). Recent surveys suggest that today’s parents are more tolerant of this, perhaps because this is becoming a more normative experience than in the past. Moreover, children who return are more likely to have had good relationships with their parents growing up, so there may be less stress between parents and their adult children who return (Sandberg-Thoma et al., 2015). Parents of young adults who have moved back home because of economic reasons report that they are just as satisfied with their life as are parents whose adult children are still living independently (Parker, 2012). Parker found that adult children age 25 and older are more likely to contribute financially to the family or complete chores and other household duties. Parker also found that living in a multigenerational household may be acting as an economic safety net for young adults. In comparison to young adults who were living outside of the home, those living with their parents were less likely to be living in poverty (17% versus 10%).
So far we have considered the impact that adult children who have returned home or have yet to leave the nest have on the lives of middle-aged parents. What about the effect on parents who have adult children dealing with personal problems, such as alcoholism, chronic health concerns, mental health issues, trouble with the law, poor social relationships, or academic or job related problems, even if they are not living at home? The life course perspective proposes the idea of linked lives (Greenfield & Marks, 2006). The notion that people in important relationships, such as children and parents, mutually influence each other’s developmental pathways. In previous chapters you have read about the effects that parents have on their children’s development, but this relationship is bidirectional. The problems faced by children, even when those children are adults, influence the lives of their parents. Greenfield and Marks found in their study of middle-aged parents and their adult children, those parents whose children were dealing with personal problems reported more negative affect, lower self-acceptance, poorer parent-child interactions, and more family relationship stress. The more problems the adult children were facing, the worse the lives and emotional health of their parents, with single parents faring the worst.
Media Attributions
- 075-Stress is licensed under a CC0 (Creative Commons Zero) license
- 074-GeneralAdaptation
- 076-WomenFriends © vilandrra is licensed under a CC BY (Attribution) license
- Sad and worried old woman © SalFalko is licensed under a CC BY-NC (Attribution NonCommercial) license
- 078-RoadRage © State Farm is licensed under a CC BY (Attribution) license
- 079-SandwichGeneration © Parker & Patton, 2013
- 079-SandwichGeneration2 © Parker & Patton, 2013
- 079-SandwichGeneration3 © Parker & Patten (2013)
