4 Mechanisms of Whiplash Injury
4.1 Proposed Theories & Presently Accepted Biomechanical Concepts for Whiplash Injury
Whiplash injuries commonly occur after an automobile accident. The victim is usually stationary and is struck from behind. A high-impact collision forces the vehicle into forward motion, with the seat taking the torso (body) and the shoulders forward with it. The head and neck, which are not as supported as the rest of the body, are thrown back due to inertia. Shortly after this, the inertia is overcome and the head and neck are thrown forwards into flexion.1,2
Efforts to explain the sequence of events, in particular the actual dynamics and motion of head and neck structures, have relied on direct and indirect evidence. Explanations for the mechanism of whiplash injury (a spectrum of identifiable and non-identifiable injuries) are extrapolated from animal studies, cadaver studies, postmortem examinations, examinations during surgery, and human volunteer studies. Historically, there have been several theories on the proposed injury mechanisms.3 One of the earlier theories, the theory of hyperextension, suggested ‘hypertranslation’ of the head as a plausible mechanism. Since the translational movement is greater at the upper cervical levels, the whiplash trauma was attributed to the cephalad portion of the cervical spine. But later experiments have consistently demonstrated the lower cervical spine as a major source of trauma.1,4,5 Other explanations included the ‘hydrodynamic theory’,3 a proposed pressure alteration inside the spinal canal as a major component; and the ‘theory of hyperextension’. Later exploratory biomechanical studies involving human volunteers and dynamic modeling have extensively investigated the kinematic response and individual motion segment analysis. These recent studies have included highspeed video cameras, accelerometers, and electromyography recordings to analyze various responses (Video 4-1). The presently accepted theory involves formation of an abnormal ‘S’ shaped curve in the cervical spine. Specifically, the cervical spine from C6 or below attains an initial position of extension.5,6 Once it reaches the maximum extension position, it forces the C5 vertebral level to extend. However, at the same time, the upper cervical spine is in a position of relative flexion, producing an S-shaped curve (Video 4-2). Normal physiological motion of the neck happens from the top downward, and hence this is considered an abnormal motion pattern. The injury to facet joints is even more severe if the head is rotated.7
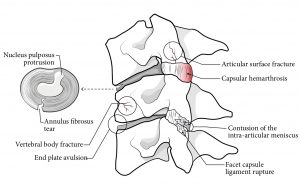
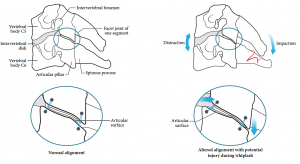
Researchers from the Medical College of Wisconsin have also proposed a kinematic-based hypothesis to explain the mechanisms applicable to the two most common complaints of whiplash patients.3 Mechanisms of headache and upper neck pain have been explained by the initial stages of acceleration causing the non-physiological flexion of the upper cervical spine, along with stretch and abnormal electrical activity of the suboccipital muscles.3 The other common complaint of lower neck pain has been explained by the pinching and resultant stretch of the lower facet joints of the cervical spine and annular tears or disc prolapse (Figure 4-1 and Figure 4-2).
4.2 References
- Slipman CW, ed. Interventional spine: An algorithmic approach. Philadelphia; PA: Saunders Elsevier; 2008:583-7.
- Eck JC, Hodges SD, Humphreys SC. Whiplash: a review of a commonly misunderstood injury. Am J Med 2001;110:651-6.
- Yoganandan N, Pintar F, Gennarelli T. Biomechanical mechanisms of whiplash injury. Traffic Inj Prev 2002;3:98-104.
- Cholewicki J, Panjabi MM, Nibu K, Babat LB, Grauer JN, Dvorak J. Head kinematics during in vitro whiplash simulation. Accid Anal Prev 1998;30:469-79.
- Grauer JN, Panjabi MM, Cholewicki J, Nibu K, Dvorak J. Whiplash produces an S-shaped curvature of the neck with hyperextension at lower levels. Spine 1997;22:2489-94.
- Ivancic PC. Facet joint and disc kinematics during simulated rear crashes with active injury prevention systems. Spine 2011;36:E1215-24.
- Kaneoka K, Ono K, Inami S, Hayashi K. Motion analysis of cervical vertebrae during whiplash loading. Spine 1999;24:763-9; discussion 70.