Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
9 Case 3-2020: A 42-year-old man with cough and chest pain
Myocarditis presenting as typical acute myocardial infarction: A case report and review of the literature. World J Clin Cases 2020; 8(2): 415-424 [PMID: 32047794 DOI: 10.12998/wjcc.v8.i2.415]
Hou YM, Han PX, Wu X, Lin JR, Zheng F, Lin L, Xu R.
Case Summary 1
A 42-year man is presented with a cough, chest pain and has a history of hypertension and smoking. Laboratory investigations of cardiac biomarkers troponin I, troponin T, and CK-MB (creatine kinase-MB) were elevated. Electrocardiogram (ECG) also showed T-wave inversion. Coronary angiography showed normal results.Cardiovascular magnetic resonance imaging (CMR) was done which shows a thicker anterior wall and FST2WI (Fat Suppressed T2-Weighted Imaging) shows edema. Rubella virus IgG and IgM antibodies were also elevated.
Learning Objectives
Investigating the clinical history of the patient and examinations to present a confirmatory diagnosis for cardiac disease.
Identifying and differentiating between the cardiac biomarkers required to assess acute myocardial infractions.
Familiarizing and defining new medical terminology associated with cardiac disease.
Clinical History 1
Age: 42 years old
Sex: Male
Medical History 1
Hypertension for 2 years. The patient has a history of smoking.
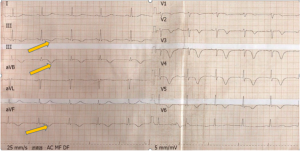
After admission, ECG was done and that showed T inversions on lead II, III, and aVF.
Figure 1: ECG shows T inversion (yellow arrows) in lead II, III, and aVF1.1
Coronary Angiography1
Normal (at day 5).
Cardiac Magnetic Resonance Imaging (MRI) 1
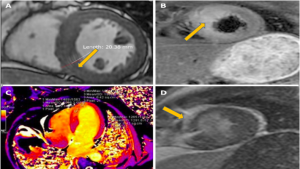
Wall motion abnormalities (mid septal, apical septal, and apical anterior), and the anterior walls were obviously thicker than the normal walls (Figure 2A), with the thickest part of the ventricular wall being approximately 20 mm.
FST2WI (Fat Suppressed T2-Weighted Imaging -Figure 2B) – Edema of the mid septal, apical septal, and apical anterior walls (Figure 2B). T1 mapping (Figure 2C) depicts more specifically myocardial edema.
Late gadolinium enhancement (LGE) (Figure 2D): shows enhancement in the endocardium and middle myocardium of the mid septal and apical septal walls.
Figure 2: Cardiovascular magnetic resonance imaging. A: In the [pb_glossary id="526"]CINE[/pb_glossary] sequence at the left ventricular end-diastolic phase, the ventricular wall (yellow arrow) was 20.38 mm (normal 12 mm). B: FS-T2WI showed obvious edema (yellow arrow); C: The T1 mapping showed that the T1 value of the walls was obviously higher than that of the normal walls (1586.3 ms vs 1291.6 ms) in the interventricular septum in the first cardiovascular magnetic resonance. D: Late gadolinium enhancement (yellow arrow) of the endocardium and middle myocardium of the middle and apical septal walls.1
Question & Answers Leading to Diagnosis:
Question 1:Based on the ECG, what cardiac biomarkers should we examine for this patient? What would they tell us?
Question 2: What is the purpose of IgG and IgM antibody analysis?
Question 3: Which tests were performed to confirm the diagnosis? How can we interpret these results?
** For answers please check the next chapter.
Medical terminology/Abbreviations:
TnI (Troponin I) – Cardiac bio marker. Cardiac troponin T (cTnT) and troponin I (cTnI) are cardiac regulatory proteins that control the calcium-mediated interaction between actin and myosin.12
IgG – Immunoglobulin G-antibody. IgG is synthesized mostly in the secondary immune response to pathogens. 13
IgM – Immunoglobulin M-antibody. It is mainly produced in the primary immune response to infectious agents or antigens.13
Brain natriuretic peptide (BNP) – Peptide hormone that is released in response to volume expansion and the increased wall stress of cardiac myocytes.2
CMR imaging – Cardiovascular magnetic resonance imaging.6
Cine CMR – Consists in the acquisition of the same slice position at different phases of the cardiac cycle. 6
FST2WI – Fat Suppressed T2-Weighted Imaging.4 FST2WI fusion technology improves signal differences with surrounding structures and facilitates the better evaluation of disease. 4
Late gadolinium enhancement – Gadolinium is a chemical agent used as a contrast, administered intravenously to achieve optimum contrast between normal and infarcted myocardium.3
T1 mapping – It is a cardiac magnetic resonance (CMR) imaging technique, which shows early clinical promise particularly in the setting of diffuse fibrosis.7
References
Hou YM, Han PX, Wu X, Lin JR, Zheng F, Lin L, Xu R. Myocarditis presenting as typical acute myocardial infarction: A case report and review of the literature. World J Clin Cases 2020; 8(2): 415-424 [PMID: 32047794 DOI: 10.12998/wjcc.v8.i2.415]
Doltra, A., Amundsen, B., Gebker, R., Fleck, E., & Kelle, S. (2013). Emerging Concepts for Myocardial Late Gadolinium Enhancement MRI. Current Cardiology Reviews, 9(3), 185-190. doi: 10.2174/1573403×113099990030
Feng, S., Huang, M., Dong, Z., Xu, L., Li, Y., & Jia, Y. et al. (2019). MRI T2-Weighted Imaging and Fat-Suppressed T2-Weighted Imaging Image Fusion Technology Improves Image Discriminability for the Evaluation of Anal Fistulas. Korean Journal Of Radiology, 20(3), 429. doi: 10.3348/kjr.2018.0260
S, G., D, P., R, O., P, F., A, F., & E, P. et al. (2021). New diagnostic criteria for acute myocardial infarction and in-hospital mortality. Retrieved 14 May 2021, from https://pubmed.ncbi.nlm.nih.gov/15861905/
Daire, J., Jacob, J., Hyacinthe, J., Croisille, P., Montet-Abou, K., & Richter, S. et al. (2008). Cine and tagged cardiovascular magnetic resonance imaging in normal rat at 1.5 T: a rest and stress study. Journal Of Cardiovascular Magnetic Resonance, 10(1), 48. doi: 10.1186/1532-429x-10-48
Yingchoncharoen, T., Jellis, C., Popovic, Z., Flamm, S., & Kwon, D. (2014). Reproducibility of multiple T1 Mapping techniques and to ECV quantification. Journal Of Cardiovascular Magnetic Resonance, 16(S1). doi: 10.1186/1532-429x-16-s1-p18
Best, J. (2002). Lesson of the week: Interpretation of rubella serology in pregnancy—pitfalls and problems. BMJ, 325(7356), 147-148. doi: 10.1136/bmj.325.7356.147
Sharma, S. (2004). Cardiac troponins. Journal Of Clinical Pathology, 57(10), 1025-1026. doi: 10.1136/jcp.2003.015420
Cardiac troponin T (cTnT) and troponin I (cTnI) are cardiac regulatory proteins that control the calcium-mediated interaction between actin and myosin.
Immunoglobulin G-antibody. IgG is synthesized mostly in the secondary immune response to pathogens.
Immunoglobulin M-antibody. It is mainly produced in the primary immune response to infectious agents or antigens.
The erythrocyte sedimentation rate (ESR or sed rate) is the rate at which red blood cells in anticoagulated whole blood descend in a standardized tube over a period of one hour.
Peptide hormone that is released in response to volume expansion and the increased wall stress of cardiac myocytes.
It is a cardiac magnetic resonance (CMR) imaging technique, which shows early clinical promise particularly in the setting of diffuse fibrosis.
Gadolinium is a chemical agent used as a contrast, administered intravenously to achieve optimum contrast between normal and infarcted myocardium.