Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
13 Case 1-2016: A 12-year-old boy with fever and recurrent abdominal pain
Wilson's Disease: A Rare Case Report in Western Maharashtra. Int J Sci Stud 2016;4(2):282-285
Pawar VS, Sontakke A, Sindal D, Patil S, Garud K.
Case Summary 1
A 12-year-old boy hailing from rural India presents with chief complaints of abdominal pain with fever for 7days. He had been having similar types of attacks every 3-4 months since he was 3 years of age and hasn’t received any proper treatment. On examination, he was conscious and well-oriented while his abdominal palpation revealed an enlarged spleen. Lab investigations revealed an abnormality in blood counts, peripheral blood film, along with very low ceruloplasmin level with a high copper concentration in urine. His brain MRI also showed some hyperintensities in the midbrain. The patient was then treated according to the diagnosisand his condition improved gradually.
Learning Objectives
Identifying the signs of suspected liver disease in children.
Recognize the clinical and laboratory findings associated with liver disease.
Describing the common clinical laboratory tests used to diagnose Wilson’s disease.
Familiarizing and defining new medical terminology associated with genetic metabolic disorders.
Clinical History 1
Age: 12 years old
Sex: Male
Medical History 1
History of recurrent episodes of abdominal pain and fever every 3-4 months since his 3 years of age.
He is a child of non-consanguineous (non-related) parents with normal developmental milestones.
Drug History 1
The patient was taken treatment for the same complaints (diagnosed as hepatitis), but details were not available.
No history of blood transfusions.
Symptoms 1
Moderate fever for 7 days.
Pain in left side of abdomen for same duration.
No history of chills, rigor, vomiting, loose motion, rash, jaundice, joint pain, chest pain, hematemesis (blood vomiting), melena (altered blood in stool).
Examinations (Clinical Assays/Tests/Imaging) 1
Physical Examination 1
The patient was conscious and well oriented.
Vital signs (pulse, blood pressure, respiratory rate) were normal.
Abdominal examination revealed a soft, non-tender spleen which was palpable 2cm below the left costal margin and hard in consistency with a smooth, regular surface. The liver was not palpable.
Neurological and psychological examinations were normal.
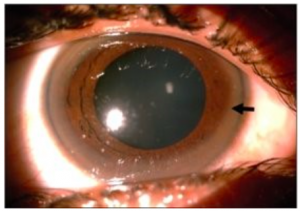
Showed a rusty brown Kayser-Fleischer (KF) ring in Descemet’s membrane of cornea near limbus of both eyes, no deposits seen on the lens. Figure 1: Slit-lamp examination showing KF ring (black arrow) 1
Laboratory Investigations 1
Complete blood count with other blood investigations was done and the results are given below.
Chart 1: Laboratory parameters1
Investigation name
Result
Hb
10.1 g/dl
WBC count
2,340 cells/cumm
Platelets
90,000/cumm
Peripheral blood film
RBC showed anisopoikilocytes (various sizes of RBC), microcytes (small RBC).
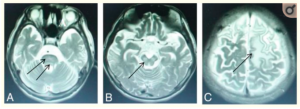
On brain MRI, T2-weighted images revealed high signal hyperintensities in the bilateral ventrolateral thalami and putamen region, midbrain, pons, cerebellum on the left side.
Figure 2: High signal intensity lesions on T2WI. Wilson disease in a 14-year-old girl with dystonia, with a diagnosis lag time of 5 years (participant group >3 years) and abnormal signal in the pons (D), midbrain (E), and frontal and parietal lobes (F) (arrows).5
Question & Answers Leading to Diagnosis:
Question 1:Based on chief complaints, medical history, physical examinations, what differential diagnoses can we suspect? Give your explanation in favor of each diagnosis.
Question 2:To confirm the diagnosis what lab investigations should be done and how would you interpret the results to confirm the diagnosis in this given case?
Question 3:If this condition remains untreated, what complications might arise and how can we follow up this patient in future?
** For answers please check the next chapter.
Medical terminology/Abbreviations:
Slit-lamp examination – A slit lamp is a microscope with a bright light used during an eye exam. It gives your ophthalmologist a closer look at the different structures at the front of the eye and inside the eye. It’s a key tool in determining the health of your eyes and detecting eye disease. 2
Kayser-Fleischer (KF) ring – Kayser–Fleischer (KF) rings are a common ophthalmologic finding in patients with Wilson disease. Initially thought to be due to the accumulation of silver, they were first demonstrated to contain copper in 1934. KF rings are seen in most of the patients with neurologic involvement from Wilson disease. These rings are caused by the deposition of excess copper on the inner surface of the cornea in the Descemet membrane. A slit-lamp examination is mandatory to make a diagnosis of KF rings particularly in the early stages unless the rings are visible to the naked eye in conditions of severe copper overload. Kayser–Fleischer rings do not cause any impairment of vision but disappear with treatment and reappear with disease progression. KF rings are not specific to Wilson disease alone, they are also seen in other chronic cholestatic disorders such as primary biliary cholangitis and children with neonatal cholestasis. 3
Ceruloplasmin test- Ceruloplasmin is a copper-containing enzyme that plays a role in the body’s iron metabolism. This test measures the amount of ceruloplasmin in the blood. The liver binds copper to a protein to produce ceruloplasmin and then releases it into the bloodstream. About 95% of the copper in the blood is bound to ceruloplasmin. Because of this, the ceruloplasmin test can be used along with one or more copper tests to help diagnose Wilson disease, an inherited disorder that can lead to excess storage of copper in the eyes, liver, brain, and other organs. 4
Brain MRI in Wilson disease- MR imaging is a sensitive method to evaluate the brains of patients with neurologic WD. Whereas abnormalities in the putamen are the most common feature of neurologic WD, brain shrinkage is also frequently observed. 5
References
Pawar VS, Sontakke A, Sindal D, Patil S, Garud K. Wilson’s Disease: A Rare Case Report in Western Maharashtra. Int J Sci Stud 2016;4(2):282-285
Yu, X., Gao, S., Yang, R., & Han, Y. (2019). MR Imaging of the Brain in Neurologic Wilson Disease. American Journal Of Neuroradiology, 40(1), 178-183. https://doi.org/10.3174/ajnr.a5936
Litwin, T., Dusek, P., Szafrański, T., Dzieżyc, K., Członkowska, A., & Rybakowski, J. (2018). Psychiatric manifestations in Wilson’s disease: possibilities and difficulties for treatment. Therapeutic Advances In Psychopharmacology, 8(7), 199-211. https://doi.org/10.1177/2045125318759461
Ceruloplasmin is a protein that is made in the liver. It stores and carries copper from the liver into the bloodstream and to the parts of your body that need it.
relating to or denoting people descended from the same ancestor.
A slit lamp is a microscope with a bright light used during an eye exam. It gives your ophthalmologist a closer look at the different structures at the front of the eye and inside the eye. It’s a key tool in determining the health of your eyes and detecting eye disease.
Kayser–Fleischer (KF) rings are a common ophthalmologic finding in patients with Wilson disease. Initially thought to be due to the accumulation of silver, they were first demonstrated to contain copper in 1934. KF rings are seen in most of the patients with neurologic involvement from Wilson disease. These rings are caused by the deposition of excess copper on the inner surface of the cornea in the Descemet membrane. A slit-lamp examination is mandatory to make a diagnosis of KF rings particularly in the early stages unless the rings are visible to the naked eye in conditions of severe copper overload. Kayser–Fleischer rings do not cause any impairment of vision but disappear with treatment and reappear with disease progression. KF rings are not specific to Wilson disease alone, they are also seen in other chronic cholestatic disorders such as primary biliary cholangitis and children with neonatal cholestasis.
Ceruloplasmin is a copper-containing enzyme that plays a role in the body's iron metabolism. This test measures the amount of ceruloplasmin in the blood. The liver binds copper to a protein to produce ceruloplasmin and then releases it into the bloodstream. About 95% of the copper in the blood is bound to ceruloplasmin. Because of this, the ceruloplasmin test can be used along with one or more copper tests to help diagnose Wilson disease, an inherited disorder that can lead to excess storage of copper in the eyes, liver, brain, and other organs.
Brain MRI in Wilson disease- MR imaging is a sensitive method to evaluate the brains of patients with neurologic WD. Whereas abnormalities in the putamen are the most common feature of neurologic WD, brain shrinkage is also frequently observed.