13.3 – Physiology (Function) of the Skeletal System
The bones of the skeletal system are comprised of an inner spongy tissue referred to as bone marrow. There are two types of bone marrow, red and yellow. The red bone marrow produces the red blood cells and it does so by a process called hematopoiesis. The yellow bone marrow contains adipose tissues which can be a source of energy. The bones of the skeletal system also store minerals such as calcium and phosphate. These minerals are important for the physiological processes in the body and are released into the bloodstream when levels are low in the body.
Joints
Watch Joints: Crash Course Anatomy & Physiology #20 (10 min) on YouTube
Media 13.2: CrashCourse. (2015, May 26). Joints: Crash Course Anatomy & Physiology #20 [Video]. YouTube. https://youtu.be/DLxYDoN634c
Most bones connect to at least one other bone in the body. The area where bones meet bones or where bones meet cartilage are called articulations. Joints can be classified based on their ability to move. At movable joints, the articulating surfaces of the adjacent bones can move smoothly against each other. However, other joints may be connected to each other by connective tissue or cartilage. These joints are designed for stability and provide for little or no movement. Importantly, joint stability and movement are related to each other. This means that stable joints allow for little or no mobility between the adjacent bones. Conversely, joints that provide the most movement between bones are the least stable.
Did You Know?
The left and right hip bones are connected by an amphiarthrosis joint.
Based on the function of joints, there are 3 types of joints:
- Synarthrosis condition of joints which allow no movement
- example: joints of the skull
- Amphiarthrosis condition of joints which allow some movement
- example: joints of the pubic symphysis
- Diarthrosis condition of joints which allow for free movement
- example: joints of the knee
Structures associated with joints are:
- Cartilage: the elastic connective tissue that is found at the ends of bones, nose tip, etc
- Synovial membrane: the lining or covering of synovial joints
- Synovial fluid: the lubricating fluid found between synovial joints
- Ligaments: the tough, elastic connective tissue that connects bone to bone
- Tendons: the fibrous connective tissue that attaches muscle to bone
- Bursa: the closed, fluid-filled sacs that work as a cushion
- Meniscus: C-shaped cartilage that act as a shock absorber between bones
Body Movements
Synovial joints are movable joints and provide most of the body movements. Body movement occurs when the bones, joints and muscles work together.
Flexion and Extension
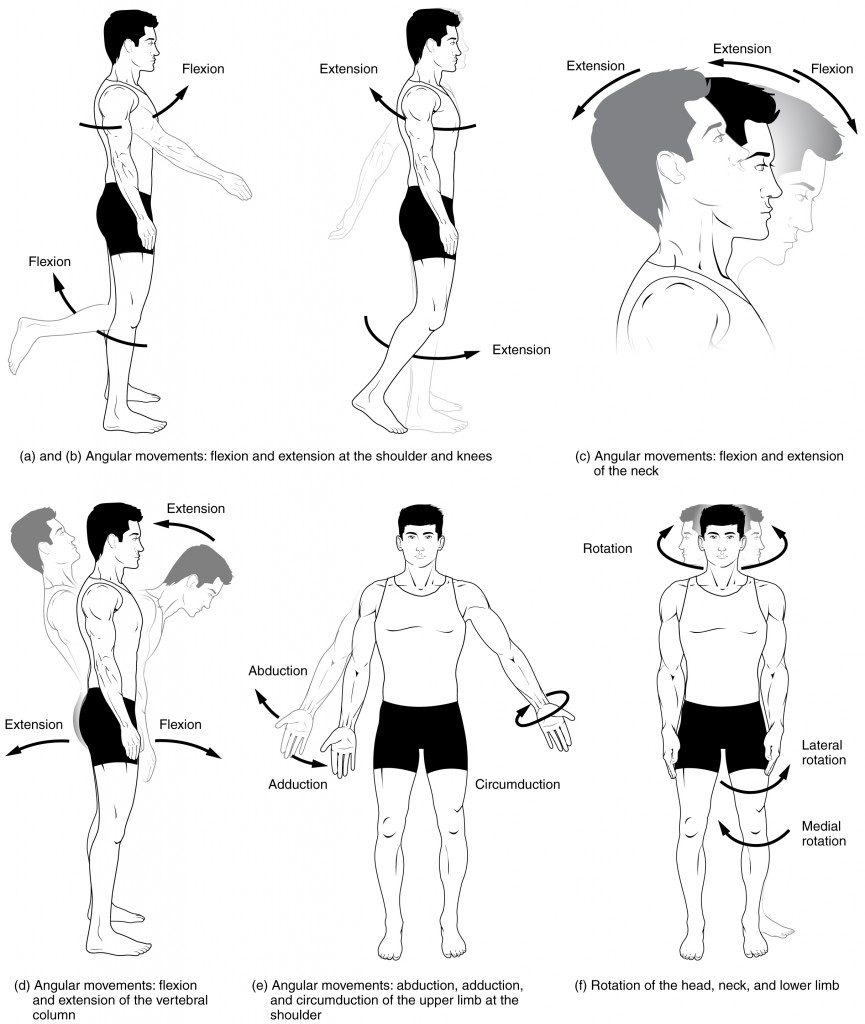
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backwards. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the joints as well as the associated intervertebral disc.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint (see Figure 13.8(a-d)). You will discover in the muscular system chapter that the associated muscles to these movements are the flexor and extensor.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body (see Figure 13.8(e)). In the muscular system chapter you will discover that the associated muscles to these movements are the abductor and adductor.
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint (see Figure 13.8(e)).
Rotation
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body (see Figure 13.8(f)).
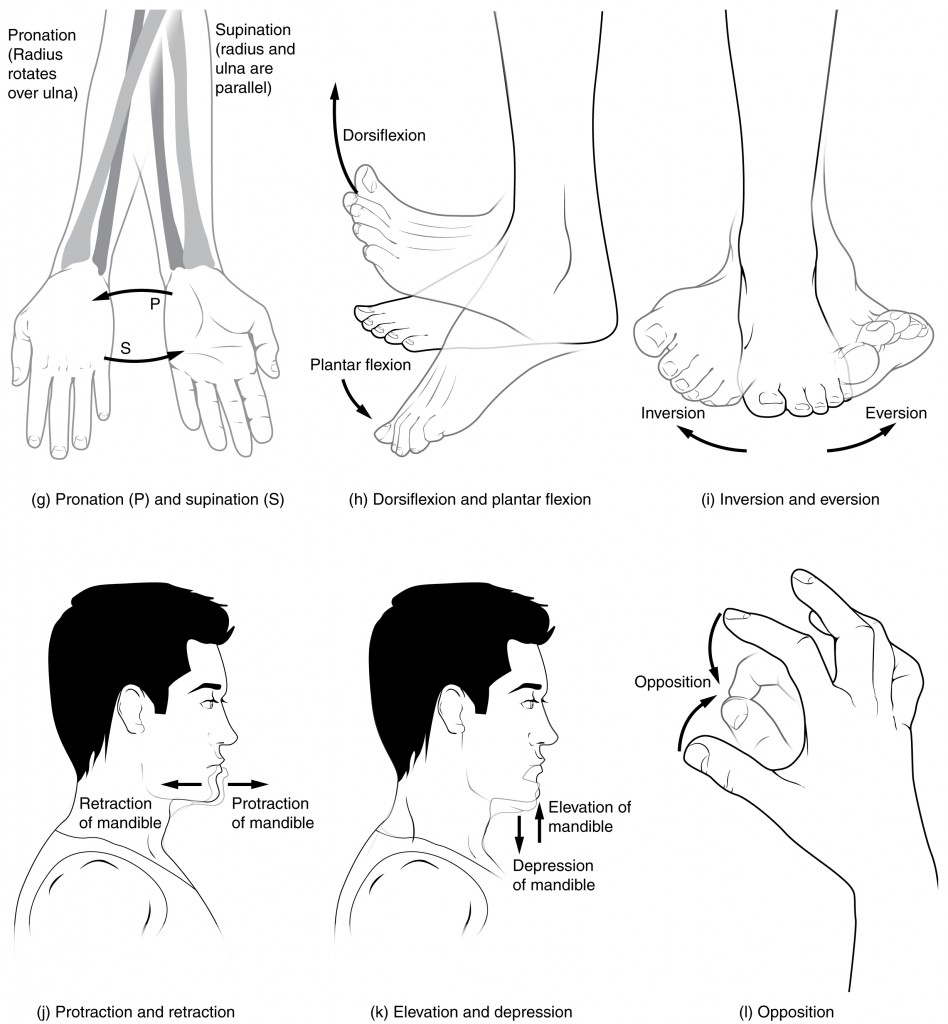
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backwards, the forearm is in the pronated position, and the radius and ulna form an X-shape.
Pronation is the movement that allows the palm of the hand to face backwards, while in supination the palm of the hand faces forwards. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 13.9(g)).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot so that the top of the foot moves (upward) toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 13.9(h)).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 13.9(i)).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward to stick out the chin, while retraction pulls the lower jaw backwards (see Figure 13.9(j)).
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, the elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces an opening of the mouth (see Figure 13.9(k)).
Concept Check
- Discuss the joints involved and movements required for you to cross your arms together in front of your chest.
- Differentiate between pronation and supination.
Musculoskeletal System Body Movements
Musculoskeletal System Body Movements (Text Version)
Practice the following endocrine system words by breaking into word parts and pronouncing.
- adduction
- moving toward the midline
- rotation
- turn around on own axis
- extension
- increased angle between bone and joint by placing a limb in a straight position
- abduction
- moving away from the midline
- inversion
- turning inward
- supination
- turn the palm up
- eversion
- turning outward
- pronation
- turn the palm down
- flexion
- decreasing the angle of a joint by bending a limb
Activity source: Musculoskeletal System Body Movements by Kimberlee Carter, from Building a Medical Terminology Foundation by Kimberlee Carter and Marie Rutherford, licensed under CC BY- 4.0. /Text version added.
Musculoskeletal System – Operative Report
Musculoskeletal System – OPERATIVE REPORT (Text version)
Using the words below fill in the operative report:
- chondromalacia
- x-rays
- arthritis
- Orthopedic
- arthroscopy
- total hip arthroplasty
- femoral
- tendinitis
PATIENT NAME: Mrs. Karen SMITH
AGE: 72 Sex: Female
DATE OF SURGERY: February 24
PREOPERATIVE DIAGNOSIS: Degenerative arthritis of both hips; more severe on the right side.
POSTOPERATIVE DIAGNOSIS: Severe degenerative arthritis and severe _________[Blank 1] of the right hip.
NAME OF PROCEDURE: Total hip arthroplasty.
HISTORY: Mrs. Karen Smith is a 72-year-old widow who has been living alone and independently since her husband’s premature death 15 years ago. Mrs. Smith has worked for 30 years at the production line in a factory and is now retired.
Mrs. Smith has been experiencing discomfort in her hips, especially the right one, over the parts twenty years or so. However, what started as a mild discomfort over time turned into severe pain. Now the pain is so bad that she is afraid that it might soon rob her of her independence. She first sought help for her hip pain many years ago. After physical examination, her family physician ordered _________[Blank 2] for both hip joints. Based on the results, it was concluded that the pain was due to severe _______[Blank 3] mainly due to wear and tear. She was advised to lose weight and to take over-the-counter painkillers as needed. She was also referred to a physiotherapist. However, despite the fact that she has lost 10% of her original body weight of 170 pounds and has been adhering to the exercise regimen recommended by her physiotherapist, the pain has grown worse over the years and now is almost unbearable. She was last visited by an orthopedic surgeon and subsequently was admitted to the General Hospital Outpatient _________[Blank 4] Clinic for ___________[Blank 5] of both hips.
OPERATIVE REPORT: The patient was brought to the operating room by anesthesia personnel. She was placed on the operating table. A Foley catheter was inserted. The patient was then placed into the lateral decubitus position with her right side up. The right lower extremity was prepped and draped in standard fashion for a ___________[Blank 6]. Dissection was carried sharply down through the soft tissue to the greater trochanter. The greater trochanter was used as a landmark to orient the remainder of the dissection which was continued posteriorly and proximally to expose the iliofemoral joint.
The acetabulum was reamed. A 50 mm acetabular shell was used. Femur was debrided using a _________[Blank 7] canal curette. The length of the femoral stem was then checked with the canal curette in place. Appropriate femoral stem and head were selected and implanted. Intraoperative radiographs were obtained to ensure proper component position.
The hip was then checked for range of motion. The patient reached 90 degrees of flexion and full extension with no instability. No abnormality was detected in the surrounding soft tissue. There was no indication of __________[Blank 8].
The area was then closed in a layered fashion. The subcutaneous tissues were closed using surgical Vicryl 5-0 sutures. An incisional VAC was placed over the wound as well. Sponge and needle counts were correct at the end of the operation. The patient tolerated the procedure well and was returned to the recovery room in good condition.
__________________________________
Michael Porter, MD, Orthopedic Surgery
Check your answers: [1]
Activity source: Musculoskeletal System – Operative Report by Saeedah Akram and Heather Scudder, from Building a Medical Terminology Foundation by Kimberlee Carter and Marie Rutherford, licensed under CC BY- 4.0. /Text version added.
Musculoskeletal System – Operative Report
Musculoskeletal System – Operative Report (Text version)
Use the words below to fill in the operative report:
- orthopedic
- supination
- colles
- carpal
- tenomyoplasty
- sterilized
- aligned
- fluoroscopy
- tenorrhaphy
- sutured
- splint
- arthralgia
- akinesia
- atrophy
PATIENT NAME: Liam PALMER
AGE: 22
SEX: Male
DOB: December 4
DATE OF ADMISSION: May 5
DATE OF PROCEDURE: May 5
ATTENDING PHYSICIAN: Michael Porter, MD, Orthopedic Surgery
PREOPERATIVE DIAGNOSIS: Fx of the distal end of radius.
POSTOPERATIVE DIAGNOSIS: Fx of the distal end of radius.
ANESTHESIA: General.
INDICATION: This 22-year-old male had been skating earlier today when he lost his balance and fell. Trying to break the fall with an outstretched arm, he landed on his right arm, breaking his wrist. Mr. Palmer was brought to the ________[Blank 1] clinic in Toronto General Hospital. The wrist has been kept in a neutral position since even a slight movement was painful. The injured area is edematous and any attempt for active or passive flexion, extension, _______[Blank 2], or pronation caused a sharp pain that shoots all the way to the right shoulder. Posterior-Anterior and lateral x-rays of the wrist and forearm confirmed ________[Blank 3] fracture of the distal end of radius with the broken piece displaced posteriorly. The _______[Blank 4] bones were intact. The patient required surgery to fix the broken bone. Although not certain at that point, there was a possibility that the patient also required __________[Blank 5].
PROCEDURE: The surgery was done under general anesthesia. The patient’s arm was placed in a proper position to allow for an easy and unobstructed access to the surgical area. The surgical area was _________[Blank 6]. A longitudinal incision was made to access the fracture. The fractured bone was realigned, and a metal plate was used to secure the _______[Blank 7] bone and restore stability. Throughout the surgery _________[Blank 8] was used to ensure proper reduction of the bone. The surrounding muscles, tendons, and ligaments were examined to ensure their integrity. There was no need for tenomyoplasty or ________[Blank 9]. Once the surgery was completed, the surgical incision was _________[Blank 10], the wrist was bandaged, and the arm was placed in a long cast to immobilize the wrist and elbow joints. The patient left the operation room in good and stable condition.
The patient was discharged from the hospital on the following day. He was scheduled for his first follow up visit in 3 weeks. At that time, the cast will be replaced with a removable wrist ________[Blank 11] and the patient will be referred to a physiotherapy clinic. Timely rehabilitation is extremely important in these types of fractures to reduce _______[Blank 12] and prevent from _______[Blank 13] and muscle _______[Blank 14].
_________________________________________
Michael Porter, MD, Orthopedic Surgery
Check your answers: [2]
Activity source: MUSCULOSKELETAL SYSTEM – OPERATIVE REPORT by Saeedha Akram and Heather Scudder, from Building a Medical Terminology Foundation by Kimberlee Carter and Marie Rutherford, licensed under CC BY- 4.0. /Text version added.
Image Descriptions
Figure 13.8 image description: This multi-part image shows different types of movements that are possible by different joints in the body. Labels read (from top, left): a and b angular movements: flexion and extension at the shoulders and knees, c) angular movements: flexion and extension of the neck (arrows pointing left and right to indicate movement). Labels (from bottom, left) read: d) angular movements: flexion and extension of the vertical column, e) angular movements abduction, adduction, and circumduction of the upper limb at the shoulder, f) rotation of the head, neck, and lower limb. [Return to Figure 13.8].
Attribution
Except where otherwise noted, this chapter is adapted from “Skeletal System” in Building a Medical Terminology Foundation by Kimberlee Carter and Marie Rutherford, licensed under CC BY 4.0. / A derivative of Betts et al., which can be accessed for free from Anatomy and Physiology (OpenStax). Adaptations: dividing Skeletal System chapter content into sub-chapters.
- 1.chondromalacia, 2.x-rays, 3.arthritis, 4.Orthopedic, 5.arthroscopy, 6. total hip arthroplasty, 7.femoral, 8.tendinitis ↵
- 1.orthopedic, 2.supination, 3.Colles, 4.carpal, 5.tenomyoplasty, 5.sterilized, 6.aligned, 7.fluoroscopy, 8.tenorrhaphy, 9.sutured, 10.splint, 11.arthralgia, 12.akinesia, 13.atrophy ↵
The process in which the body produces blood.
Also known as joints. It is where bones meet bones or bones meet joints.
away from the midline of the body
Movement toward the midline of the body
