The Complete Subjective Health Assessment
The complete subjective health assessment is commonly referred to as a health history. It provides an overview of the client’s current and past health and illness state. You conduct it by interviewing the client as illustrated in Figure 1.1, asking them questions, and listening to their narrative.

This information is often shared verbally with you or in the way that the client can best communicate. It is also sometimes collected through a standardized form that the client completes. In some cases, it also includes information shared by a family member, friend, or another health professional when the client is unable to communicate.
Points of Consideration
Clients are sometimes accompanied by care partners. Care partners are family and friends who are involved in helping to care for the client. You may hear care partners being referred to as “informal caregivers” or “family caregivers,” but “care partner” is a more inclusive term that acknowledges the energy, work, and importance of their role.
The complete subjective health assessment is part of assessment, the first component of the nursing process (assessment, analysis/diagnosis, planning, implementation and evaluation) outlined in Figure 1.2.
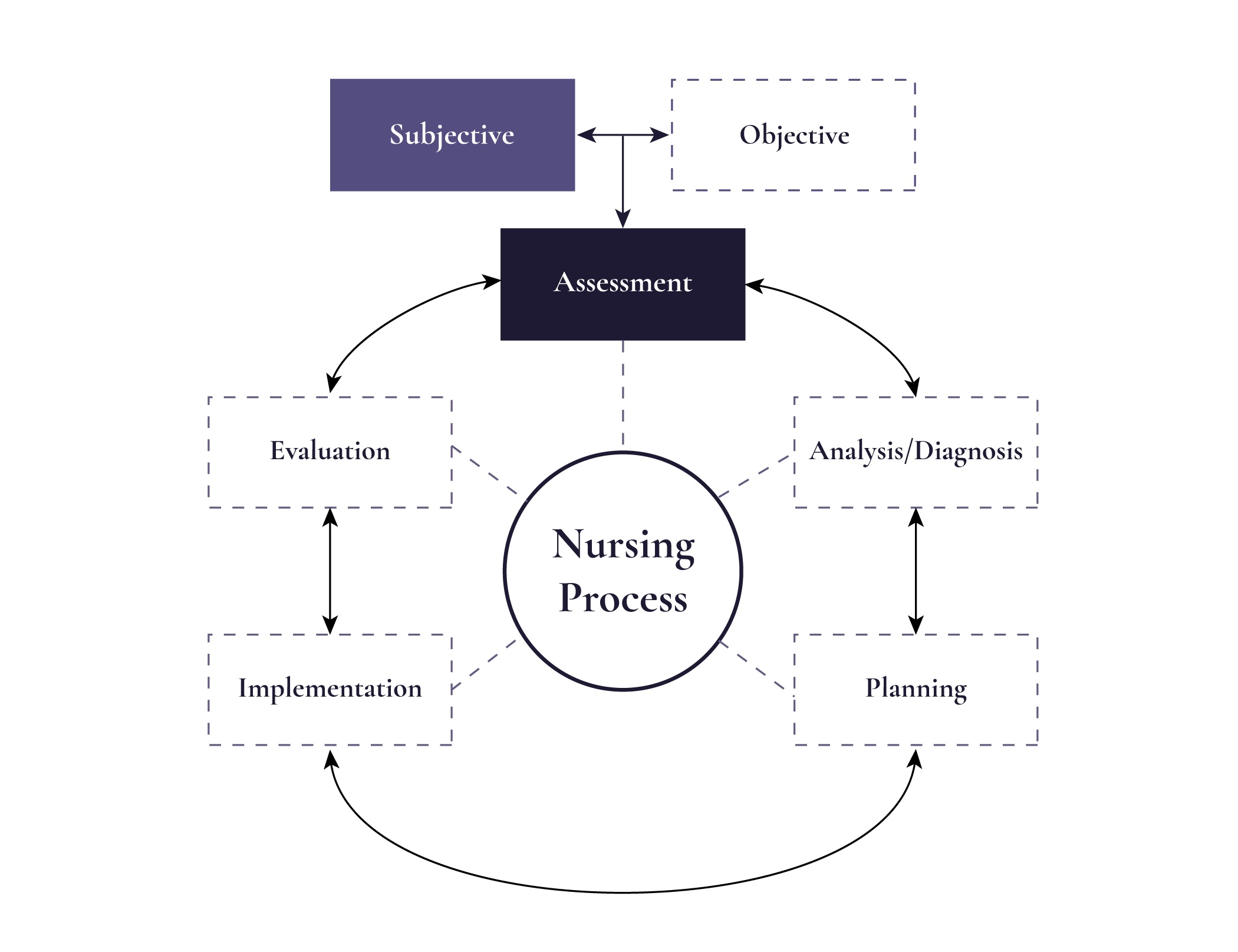
As illustrated in Figure 1.2, the assessment phase of the nursing process involves collecting subjective data (information that the client shares) and objective data (information that you collect when performing a physical exam). See Table 1.1 for an overview and examples of subjective and objective data. This book focuses on subjective data collection in the context of the complete subjective health assessment.
| Data | Example |
|
Subjective Information that the client shares with you spontaneously or in response to your questions.
|
|
|
Objective Information that you observe when conducting a physical assessment, and lab and diagnostic results.
|
|
Table 1.1: Overview and examples of subjective and objective data
As the word “subjective” suggests, this type of data refers to information that is spontaneously shared with you by the client or is in response to questions that you ask the client. Subjective data can include information about both symptoms and signs. In the context of subjective data, symptoms are something that the client feels, as illustrated in Figure 1.3 (e.g., nausea, pain, fatigue). You won’t know about a symptom unless the client tells you. Signs are something that the health professional can observe, such as a rash, bruising, or skin perspiration, also illustrated in Figure 1.3. Although you can observe signs, in the context of a subjective assessment, the client shares this subjective information with you. For example, a rash is both subjective and objective data as it could be something that the client shares with you, but it is also something that you can observe. On the other hand, if the client says that the rash is itchy, that would be considered subjective data and, in this case, it would be a symptom because it is something the client feels and you can’t observe.

Test Yourself
A term often used in reference to, or in place of, the complete subjective health assessment.
Care partners are family and friends who are involved in helping to care for the client
Information that the client shares with the health professional.
Information that the health professional collects when performing a physical exam.
Something that the client feels.
Something that the health professional observes.
