6.1 The Pectoral Girdle
Learning Objectives
By the end of this section, you will be able to:
- Describe the bones that form the pectoral girdle
- List the functions of the pectoral girdle
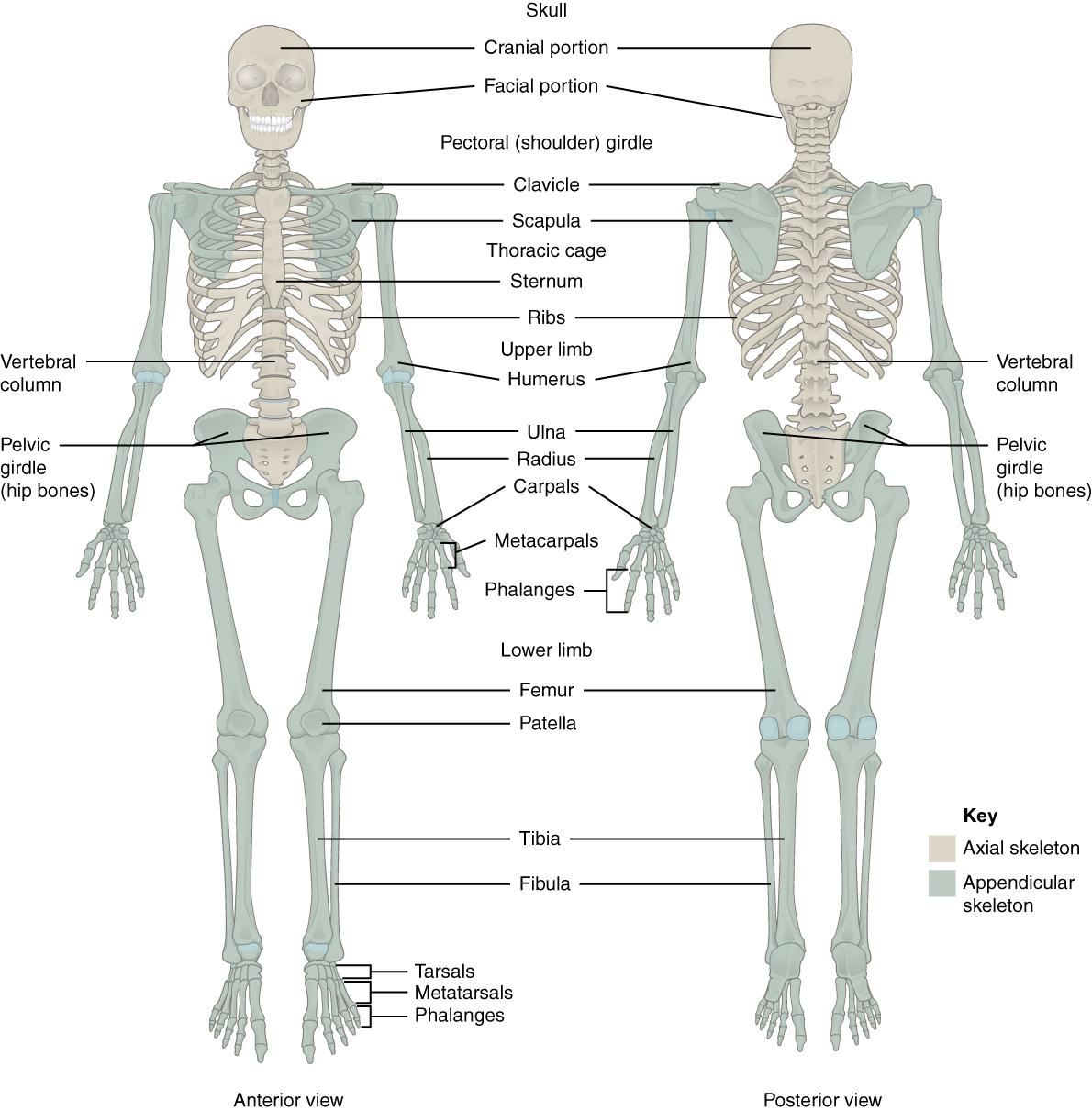
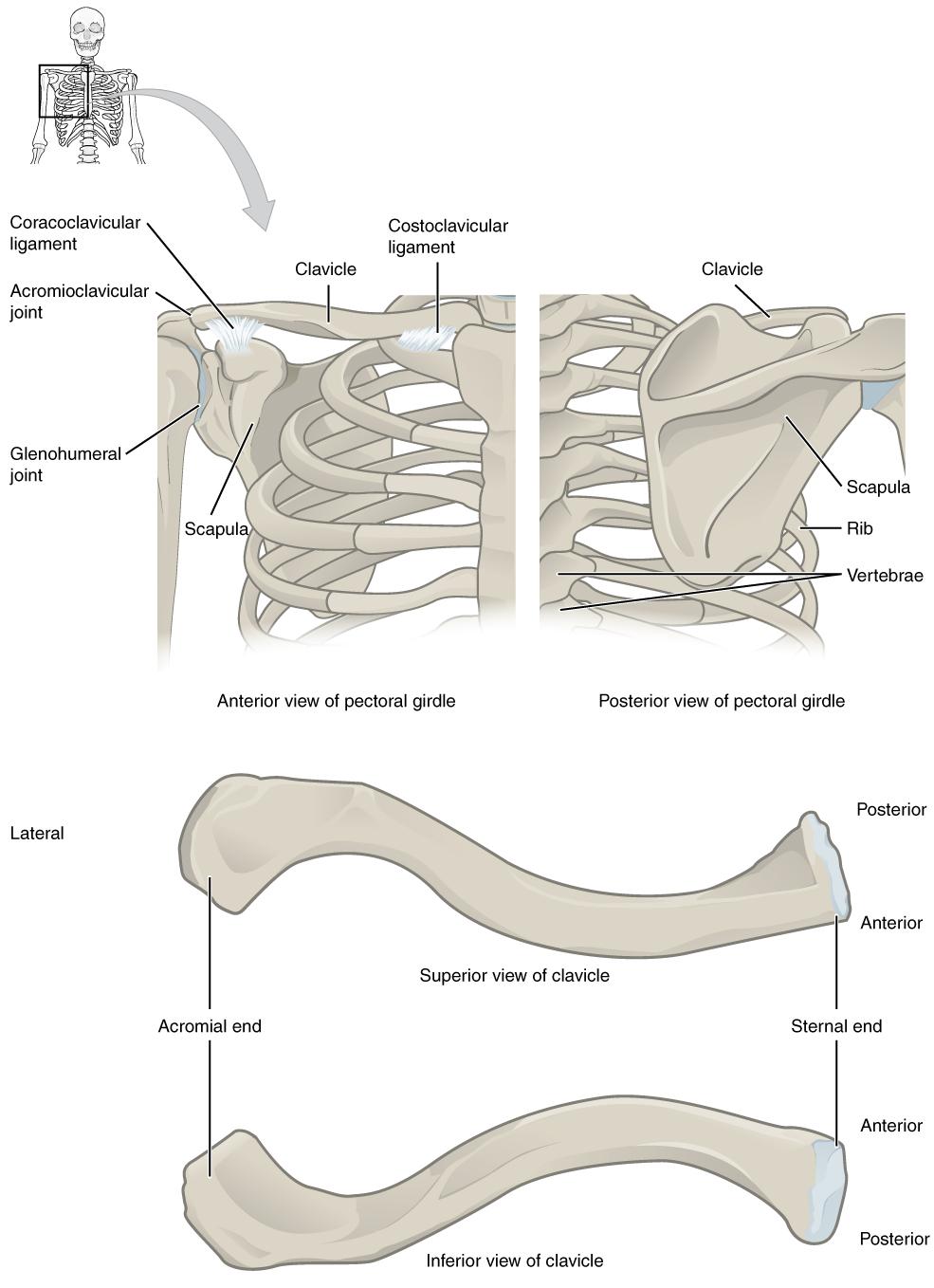
The appendicular skeleton includes all of the limb bones, plus the bones that unite each limb with the axial skeleton (Figure 6.2). The bones that attach each upper limb to the axial skeleton form the pectoral girdle (shoulder girdle). This consists of two bones, the scapula and clavicle (Figure 6.3). The clavicle (collarbone) is an S-shaped bone located on the anterior side of the shoulder. It is attached on its medial end to the sternum of the thoracic cage, which is part of the axial skeleton. The lateral end of the clavicle articulates (joins) with the scapula just above the shoulder joint. You can easily palpate, or feel with your fingers, the entire length of your clavicle.
The scapula (shoulder blade) lies on the posterior aspect of the shoulder. It is supported by the clavicle and articulates with the humerus (arm bone) to form the shoulder joint. The scapula is a flat, triangular-shaped bone with a prominent ridge running across its posterior surface. This ridge extends out laterally, where it forms the bony tip of the shoulder and joins with the lateral end of the clavicle. By following along the clavicle, you can palpate out to the bony tip of the shoulder, and from there, you can move back across your posterior shoulder to follow the ridge of the scapula. Move your shoulder around and feel how the clavicle and scapula move together as a unit. Both of these bones serve as important attachment sites for muscles that aid with movements of the shoulder and arm.
The right and left pectoral girdles are not joined to each other, allowing each to operate independently. In addition, the clavicle of each pectoral girdle is anchored to the axial skeleton by a single, highly mobile joint. This allows for the extensive mobility of the entire pectoral girdle, which in turn enhances movements of the shoulder and upper limb.
Clavicle
The clavicle is the only long bone that lies in a horizontal position in the body (see Figure 6.3). The clavicle has several important functions. First, anchored by muscles from above, it serves as a strut that extends laterally to support the scapula. This in turn holds the shoulder joint superiorly and laterally from the body trunk, allowing for maximal freedom of motion for the upper limb. The clavicle also transmits forces acting on the upper limb to the sternum and axial skeleton. Finally, it serves to protect the underlying nerves and blood vessels as they pass between the trunk of the body and the upper limb.
The clavicle has three regions: the medial end, the lateral end, and the shaft. The medial end, known as the sternal end of the clavicle, has a triangular shape and articulates with the manubrium portion of the sternum. This forms the sternoclavicular joint, which is the only bony articulation between the pectoral girdle of the upper limb and the axial skeleton. This joint allows considerable mobility, enabling the clavicle and scapula to move in upward/downward and anterior/posterior directions during shoulder movements. The sternoclavicular joint is indirectly supported by the costoclavicular ligament (costo- = “rib”), which spans the sternal end of the clavicle and the underlying first rib. The lateral or acromial end of the clavicle articulates with the acromion of the scapula, the portion of the scapula that forms the bony tip of the shoulder. There are some sex differences in the morphology of the clavicle. In women, the clavicle tends to be shorter, thinner, and less curved. In men, the clavicle is heavier and longer, and has a greater curvature and rougher surfaces where muscles attach, features that are more pronounced in manual workers.
The clavicle is the most commonly fractured bone in the body. Such breaks often occur because of the force exerted on the clavicle when a person falls onto his or her outstretched arms, or when the lateral shoulder receives a strong blow. Because the sternoclavicular joint is strong and rarely dislocated, excessive force results in the breaking of the clavicle, usually between the middle and lateral portions of the bone. If the fracture is complete, the shoulder and lateral clavicle fragment will drop due to the weight of the upper limb, causing the person to support the sagging limb with their other hand. Muscles acting across the shoulder will also pull the shoulder and lateral clavicle anteriorly and medially, causing the clavicle fragments to override. The clavicle overlies many important blood vessels and nerves for the upper limb, but fortunately, due to the anterior displacement of a broken clavicle, these structures are rarely affected when the clavicle is fractured.
Scapula
The scapula is also part of the pectoral girdle and thus plays an important role in anchoring the upper limb to the body. The scapula is located on the posterior side of the shoulder. It is surrounded by muscles on both its anterior (deep) and posterior (superficial) sides, and thus does not articulate with the ribs of the thoracic cage.
The scapula has several important landmarks (Figure 6.4). The three margins or borders of the scapula, named for their positions within the body, are the superior border of the scapula, the medial border of the scapula, and the lateral border of the scapula. The suprascapular notch is located lateral to the midpoint of the superior border. The corners of the triangular scapula, at either end of the medial border, are the superior angle of the scapula, located between the medial and superior borders, and the inferior angle of the scapula, located between the medial and lateral borders. The inferior angle is the most inferior portion of the scapula, and is particularly important because it serves as the attachment point for several powerful muscles involved in shoulder and upper limb movements. The remaining corner of the scapula, between the superior and lateral borders, is the location of the glenoid cavity (glenoid fossa). This shallow depression articulates with the humerus bone of the arm to form the glenohumeral joint (shoulder joint). The small bony bumps located immediately above and below the glenoid cavity are the supraglenoid tubercle and the infraglenoid tubercle, respectively. These provide attachments for muscles of the arm.
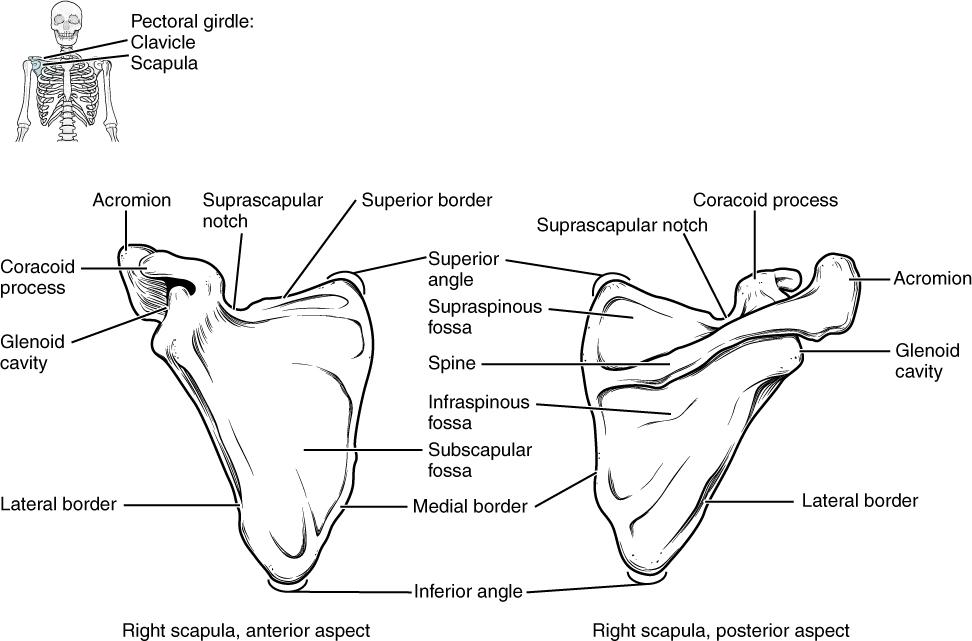
The scapula also has two prominent projections. Toward the lateral end of the superior border, between the suprascapular notch and glenoid cavity, is the hook-like coracoid process (coracoid = “shaped like a crow’s beak”). This process projects anteriorly and curves laterally. At the shoulder, the coracoid process is located inferior to the lateral end of the clavicle. It is anchored to the clavicle by a strong ligament, and serves as the attachment site for muscles of the anterior chest and arm. On the posterior aspect, the spine of the scapula is a long and prominent ridge that runs across its upper portion. Extending laterally from the spine is a flattened and expanded region called the acromion or acromial process. The acromion forms the bony tip of the superior shoulder region and articulates with the lateral end of the clavicle, forming the acromioclavicular joint (see Figure 6.3). Together, the clavicle, acromion, and spine of the scapula form a V-shaped bony line that provides for the attachment of neck and back muscles that act on the shoulder, as well as muscles that pass across the shoulder joint to act on the arm.
The scapula has three depressions, each of which is called a fossa (plural = fossae). Two of these are found on the posterior scapula, above and below the scapular spine. Superior to the spine is the narrow supraspinous fossa, and inferior to the spine is the broad infraspinous fossa. The anterior (deep) surface of the scapula forms the broad subscapular fossa. All of these fossae provide large surface areas for the attachment of muscles that cross the shoulder joint to act on the humerus.
The acromioclavicular joint transmits forces from the upper limb to the clavicle. The ligaments around this joint are relatively weak. A hard fall onto the elbow or outstretched hand can stretch or tear the acromioclavicular ligaments, resulting in a moderate injury to the joint. However, the primary support for the acromioclavicular joint comes from a very strong ligament called the coracoclavicular ligament (see Figure 6.3). This connective tissue band anchors the coracoid process of the scapula to the inferior surface of the acromial end of the clavicle and thus provides important indirect support for the acromioclavicular joint.
Following a strong blow to the lateral shoulder, such as when a hockey player is driven into the boards, a complete dislocation of the acromioclavicular joint can result. In this case, the acromion is thrust under the acromial end of the clavicle, resulting in ruptures of both the acromioclavicular and coracoclavicular ligaments. The scapula then separates from the clavicle, with the weight of the upper limb pulling the shoulder downward. This dislocation injury of the acromioclavicular joint is known as a “shoulder separation” and is common in contact sports such as hockey, football, or martial arts.
Interactive Link
Watch this video that reviews many of the anatomical landmarks of the pectoral girdle with a 3D model.
