Learning Objectives
By the end of this section, you will be able to:
Describe the layers of the skin and the functions of each layer
- Identify the components of the integumentary system
- Describe the layers of the skin and the functions of each layer
- Describe the layers of the epidermis and dermis
- Identify and describe the hypodermis and fascia
- Describe the role of keratinocytes and their life cycle
- Describe the role of melanocytes in skin pigmentation
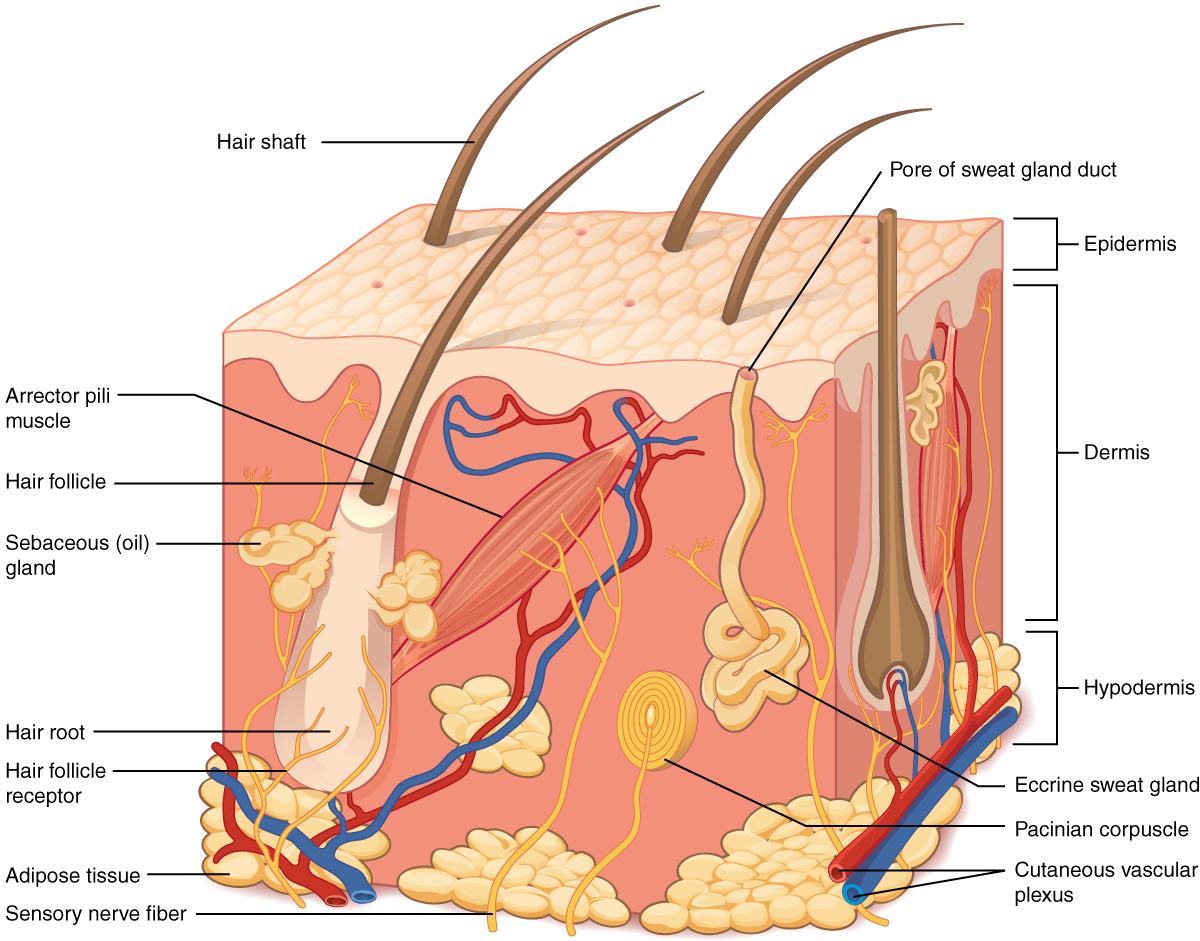
Although you may not typically think of the skin as an organ, it is in fact made of tissues that work together as a single structure to perform unique and critical functions. The skin and its accessory structures make up the integumentary system, which provides the body with overall protection. The skin is made of multiple layers of cells and tissues, which are held to underlying structures by connective tissue (Figure 5.1.1). The most superficial layer of the skin is the epidermis which is attached to the deeper dermis. Accessory structures, hair, glands, and nails, are found associated with the skin. The deeper layer of skin is well vascularized (has numerous blood vessels) and is superficial to the hypodermics. It also has numerous sensory, and autonomic and sympathetic nerve fibers ensuring communication to and from the brain.
External Website

View this animation to learn more about layers of the skin.
The skin consists of two main layers and a closely associated layer. View this animation to learn more about layers of the skin. What are the basic functions of each of these layers?
The Epidermis
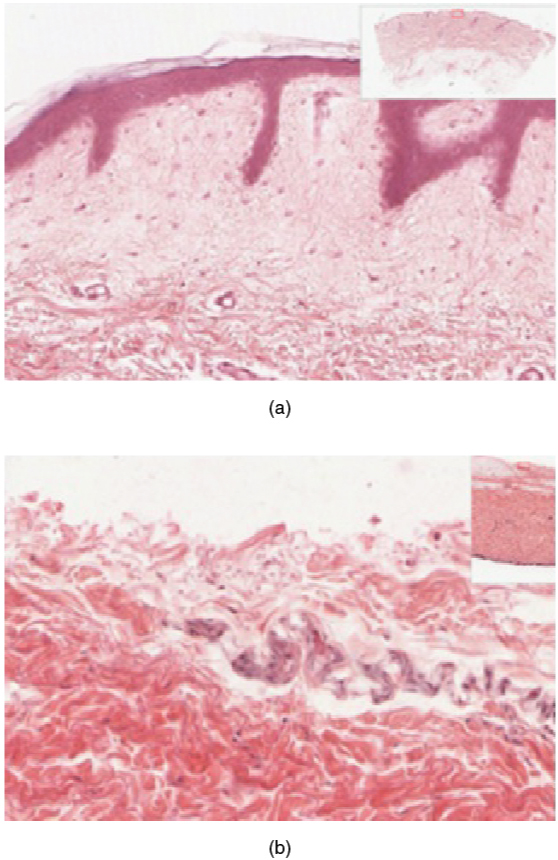
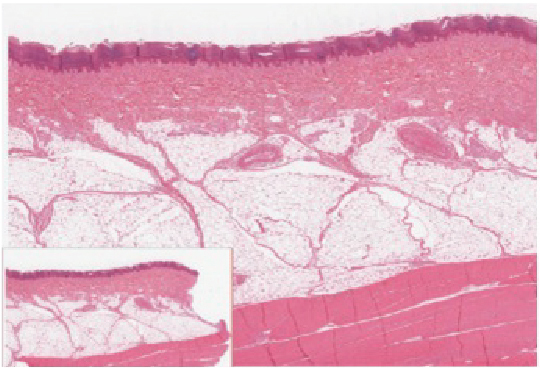
The epidermis is composed of keratinized, stratified squamous epithelium. It is made of four or five layers of epithelial cells, depending on its location in the body. It does not have any blood vessels within it (i.e., it is avascular). Skin that has four layers of cells is referred to as “thin skin.” From deep to superficial, these layers are the stratum basale, stratum spinosum, stratum granulosum, and stratum corneum. Most of the skin can be classified as thin skin. “Thick skin” is found only on the palms of the hands and the soles of the feet. It has a fifth layer, called the stratum lucidum, located between the stratum corneum and the stratum granulosum (Figure 5.1.2).
The cells in all of the layers except the stratum basale are called keratinocytes, which make up about 95% of all epidermal cells. A keratinocyte is a cell that manufactures and stores the protein keratin. Keratin is an intracellular fibrous protein that gives hair, nails, and skin their hardness, strength, and water-resistant properties. The keratinocytes in the stratum corneum are dead and regularly slough away, being replaced by cells from the deeper layers (Figure 5.1.3).
Stratum Basale
The stratum basale (also called the stratum germinativum) is the deepest epidermal layer and attaches the epidermis to the basal lamina, below which lie the layers of the dermis. The cells in the stratum basale bond to the dermis via intertwining collagen fibers, referred to as the basement membrane. (Figure 5.1.4).
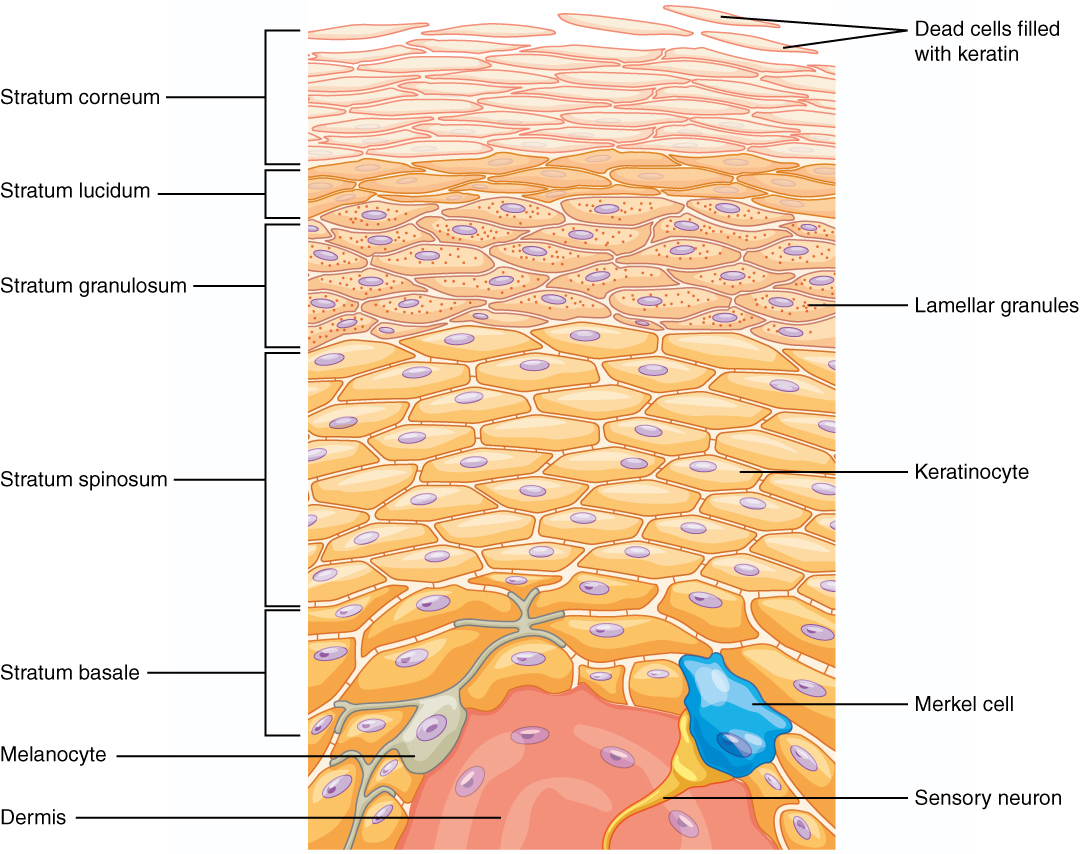
The stratum basale is a single layer of cells primarily made of basal cells. A basal cell is a cuboidal-shaped stem cell that is a precursor of the keratinocytes of the epidermis. All of the keratinocytes are produced from this single layer of cells, which are constantly going through mitosis to produce new cells. As new cells are formed, the existing cells are pushed superficially away from the stratum basale. Two other cell types are found dispersed among the basal cells in the stratum basale. The first is a Merkel cell, which functions as a receptor and is responsible for stimulating sensory nerves that the brain perceives as touch. These cells are especially abundant on the surfaces of the hands and feet. The second is a melanocyte, a cell that produces the pigment melanin. Melanin gives hair and skin its color, and also helps protect the DNA in the nuclei of living cells of the epidermis from ultraviolet (UV) radiation damage.
Stratum Spinosum
As the name suggests, the stratum spinosum is spiny in appearance due to the protruding cell processes that join the cells via a structure called a desmosome. The desmosomes interlock with each other and strengthen the bond between the cells. The stratum spinosum is composed of eight to 10 layers of keratinocytes, formed as a result of cell division in the stratum basale (Figure 5.1.5). Interspersed among the keratinocytes of this layer is a type of dendritic cell called the Langerhans cell, which functions as a macrophage by engulfing bacteria, foreign particles, and damaged cells that occur in this layer.
External Website

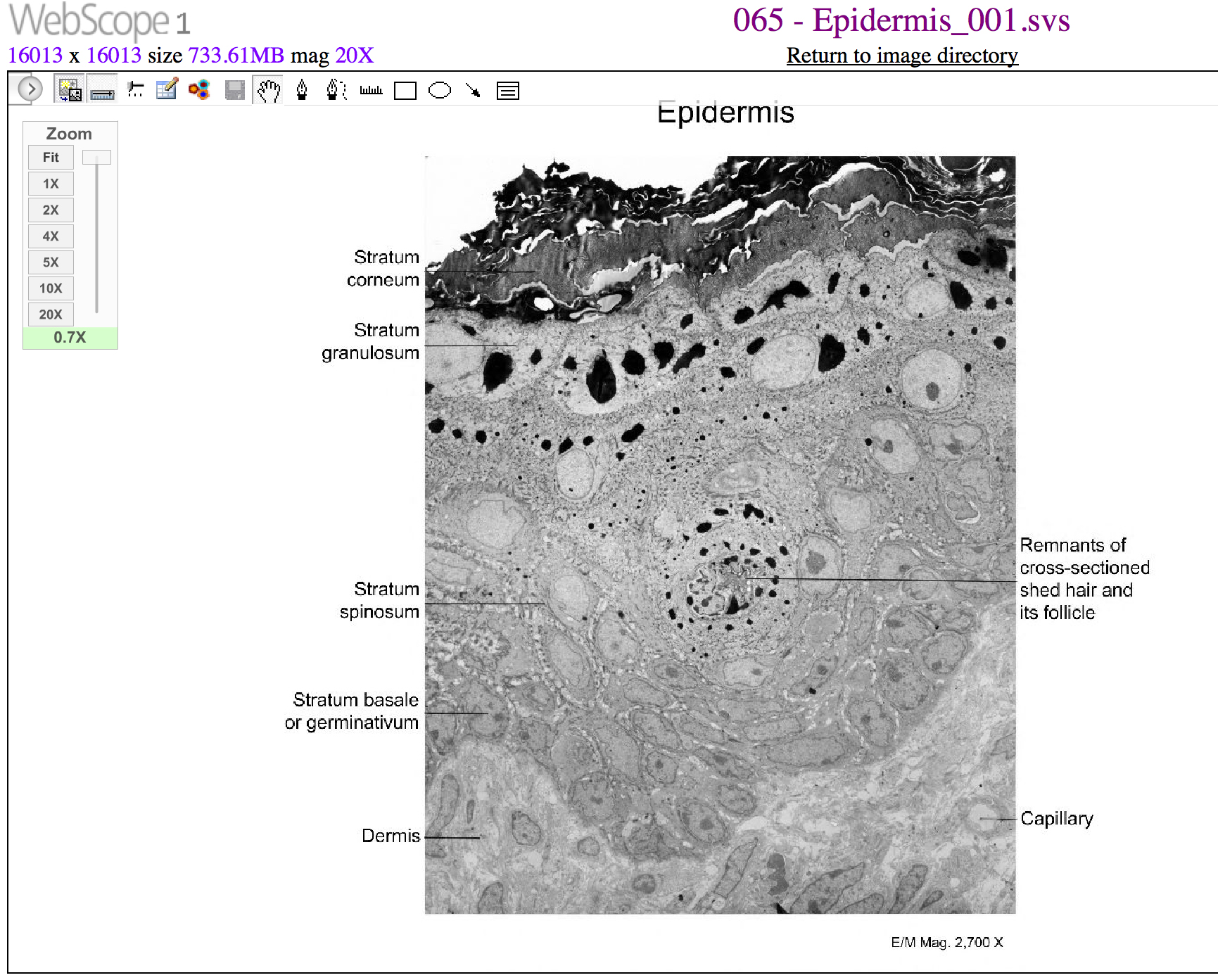
View the University of Michigan WebScope at http://virtualslides.med.umich.edu/Histology/EMsmallCharts/3%20Image%20Scope%20finals/065%20-%20Epidermis_001.svs/view.apml to explore the tissue sample in greater detail. If you zoom on the cells at the outermost layer of this section of skin, what do you notice about the cells?
The keratinocytes in the stratum spinosum begin the synthesis of keratin and release a water-repelling glycolipid that helps prevent water loss from the body, making the skin relatively waterproof. As new keratinocytes are produced atop the stratum basale, the keratinocytes of the stratum spinosum are pushed into the stratum granulosum.
Stratum Granulosum
The stratum granulosum has a grainy appearance due to further changes to the keratinocytes as they are pushed from the stratum spinosum. The cells (three to five layers deep) become flatter, their cell membranes thicken, and they generate large amounts of the proteins keratin, which is fibrous, and keratohyalin, which accumulates as lamellar granules within the cells (see Figure 5.1.4). These two proteins make up the bulk of the keratinocyte mass in the stratum granulosum and give the layer its grainy appearance. The nuclei and other cell organelles disintegrate as the cells die, leaving behind the keratin, keratohyalin, and cell membranes that will form the stratum lucidum, and the stratum corneum. A similar process of producing cells packed with keratin occurs in the accessory structures of hair and nails.
Stratum Lucidum
The stratum lucidum is a smooth, seemingly translucent layer of the epidermis located just above the stratum granulosum and below the stratum corneum. This thin layer of cells is found only in the thick skin of the palms, soles, and digits. The keratinocytes that compose the stratum lucidum are dead and flattened (see Figure 5.1.4). These cells are densely packed with eleiden, a clear protein rich in lipids, derived from keratohyalin, which gives these cells their transparent (i.e., lucid) appearance and provides a barrier to water.
Stratum Corneum
The stratum corneum is the most superficial layer of the epidermis and is the layer exposed to the outside environment (see Figure 5.1.4). The increased keratinization (also called cornification) of the cells in this layer gives it its name. There are usually 15 to 30 layers of cells in the stratum corneum. This dry, dead layer helps prevent the penetration of microbes and the dehydration of underlying tissues, and provides a mechanical protection against abrasion for the more delicate, underlying layers. Cells in this layer are shed periodically and are replaced by cells pushed up from the stratum granulosum (or stratum lucidum in the case of the palms and soles of feet). The cells in this layer can still be anchored to each other by desmosomes which is why the peeling that occurs with a sunburn peels the damaged epidermal layers in one sheet. The entire layer is replaced during a period of about 4 weeks. Cosmetic procedures, such as microdermabrasion, help remove some of the dry, upper layer and aim to keep the skin looking “fresh” and healthy.
Dermis
The dermis might be considered the “core” of the integumentary system (derma- = “skin”), as distinct from the epidermis (epi- = “upon” or “over”) and hypodermis (hypo- = “below”). It contains blood and lymph vessels, nerves, and other structures, such as hair follicles and sweat glands. The epidermis is avascular and cells of this layer must get their oxygen and nutrients from capillaries in the dermis. The dermis is made of two layers of connective tissue that compose an interconnected mesh of elastin and collagenous fibers, produced by fibroblasts (Figure 5.1.6). The more superficial papillary layer serves as an anchor point for the epidermis above and is intimately connected to the deeper reticular layer.

Papillary Layer
The papillary layer is made of loose, areolar connective tissue, which means the collagen and elastin fibers of this layer form a loose mesh with abundant ground substance supporting the hydration of the skin. This superficial layer of the dermis projects into the stratum basale of the epidermis to form finger-like dermal papillae (see Figure 5.1.6). Within the papillary layer are fibroblasts, a small number of fat cells (adipocytes), and an abundance of small blood vessels. In addition, the papillary layer contains phagocytes, defensive cells that help fight bacteria or other infections that have breached the skin. This layer also contains lymphatic capillaries, nerve fibers, and touch receptors called the Meissner corpuscles.
In a growing fetus, fingerprints form where the cells of the stratum basale of the epidermis meets the papillae of the underlying dermal layer (papillary layer), resulting in the formation of the ridges on your fingers that you recognize as fingerprints. Dermal papillae push up on the epidermis creating unique epidermal ridge patterns. Fingerprints are unique to each individual and are used for forensic analyses because the patterns do not change with the growth and aging processes.
Reticular Layer
Underlying the papillary layer is the much thicker reticular layer, composed of dense irregular connective tissue which resists forces in many directions attributing to the flexibility of the skin. This layer makes up around 80% of the dermis and is well vascularized and has a rich sensory and sympathetic nerve supply. The reticular layer appears reticulated (net-like) due to a tight meshwork of fibers. Elastin fibers provide some elasticity to the skin, enabling movement. Collagen fibers provide structure and tensile strength, with strands of collagen extending into both the papillary layer and the hypodermis. In addition, collagen binds water to keep the skin hydrated. Collagen injections and Retin-A creams help restore skin turgor by either introducing collagen externally or stimulating blood flow and repair of the dermis, respectively.
Hypodermis
The hypodermis (also called the subcutaneous layer or superficial fascia) is a layer directly below the dermis and serves to connect the skin to the underlying fascia (fibrous tissue) surrounding the muscles. It is not strictly a part of the skin, although the border between the hypodermis and dermis can be difficult to distinguish. The hypodermis consists of well-vascularized, loose, areolar connective tissue and abundant adipose tissue, which functions as a mode of fat storage and provides insulation and cushioning for the integument. Fascia is a thick connective tissue wrapping that surrounds skeletal muscles anchoring them to surrounding tissues and investing groups of muscles.
Everyday Connection – Lipid Storage
The hypodermis is home to most of the fat that concerns people when they are trying to keep their weight under control. Adipose tissue present in the hypodermis consists of fat-storing cells called adipocytes. This stored fat can serve as an energy reserve, insulate the body to prevent heat loss, and act as a cushion to protect underlying structures from trauma.
Where the fat is deposited and accumulates within the hypodermis depends on hormones (testosterone, estrogen, insulin, glucagon, leptin, and others), as well as genetic factors. Fat distribution changes as our bodies mature and age. Men tend to accumulate fat in different areas (neck, arms, lower back, and abdomen) than do women (breasts, hips, thighs, and buttocks). The body mass index (BMI) is often used as a measure of fat, although this measure is, in fact, derived from a mathematical formula that compares body weight (mass) to height. Therefore, its accuracy as a health indicator can be called into question in individuals who are extremely physically fit.
In many animals, there is a pattern of storing excess calories as fat to be used in times when food is not readily available. In much of the developed world, insufficient exercise coupled with the ready availability and consumption of high-calorie foods have resulted in unwanted accumulations of adipose tissue in many people. Although periodic accumulation of excess fat may have provided an evolutionary advantage to our ancestors, who experienced unpredictable bouts of famine, it is now becoming chronic and considered a major health threat. Recent studies indicate that a distressing percentage of our population is overweight and/or clinically obese. Not only is this a problem for the individuals affected, but it also has a severe impact on our healthcare system. Changes in lifestyle, specifically in diet and exercise, are the best ways to control body fat accumulation, especially when it reaches levels that increase the risk of heart disease and diabetes.
Pigmentation
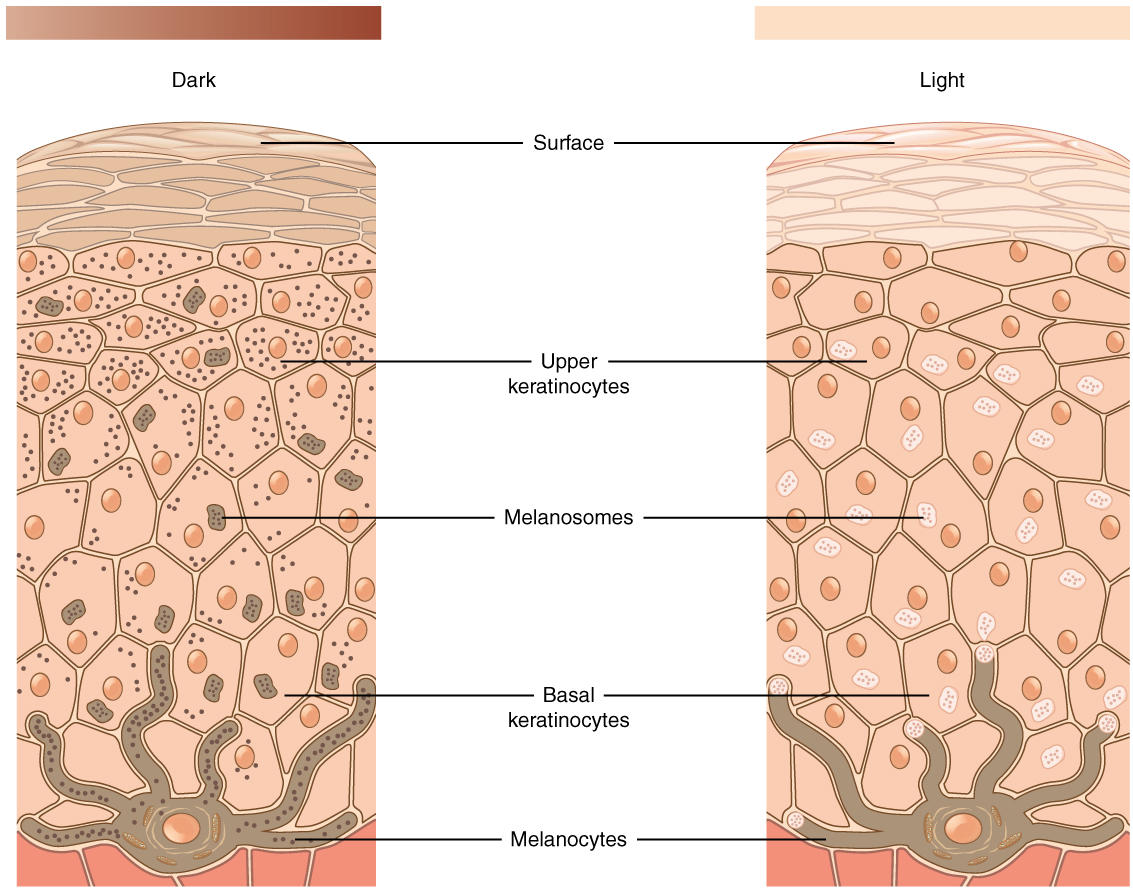
The color of skin is influenced by a number of pigments, including melanin, carotene, and hemoglobin. Recall that melanin is produced by cells called melanocytes, which are found scattered throughout the stratum basale of the epidermis. The melanin is transferred into the keratinocytes via a cellular vesicle called a melanosome (Figure 5.1.7).
Melanin occurs in two primary forms. Eumelanin exists as black and brown, whereas pheomelanin provides a red color. Dark-skinned individuals produce more melanin than those with pale skin. Exposure to the UV rays of the sun or a tanning salon causes melanin to be manufactured and built up in keratinocytes, as sun exposure stimulates keratinocytes to secrete chemicals that stimulate melanocytes. The accumulation of melanin in keratinocytes results in the darkening of the skin, or a tan. This increased melanin accumulation protects the DNA of epidermal cells from UV ray damage and the breakdown of folic acid, a nutrient necessary for our health and well-being. In contrast, too much melanin can interfere with the production of vitamin D, an important nutrient involved in calcium absorption. There is a dynamic interplay between the amount of protection from UV radiation that melanin provides and the amount of vitamin D produced. The amount of melanin produced, and therefore UV protection, is directly correlated with the amount of sunlight exposure. The more sunlight, the more UV protection, but the compromise is that with increased melanin there is a decrease in vitamin D produced.
It requires about 10 days after initial sun exposure for melanin synthesis to peak, which is why pale-skinned individuals tend to suffer sunburns of the epidermis initially. Dark-skinned individuals can also get sunburns, but are more protected than are pale-skinned individuals. Melanosomes are temporary structures that are eventually destroyed by fusion with lysosomes; this fact, along with melanin-filled keratinocytes in the stratum corneum sloughing off, makes tanning impermanent.
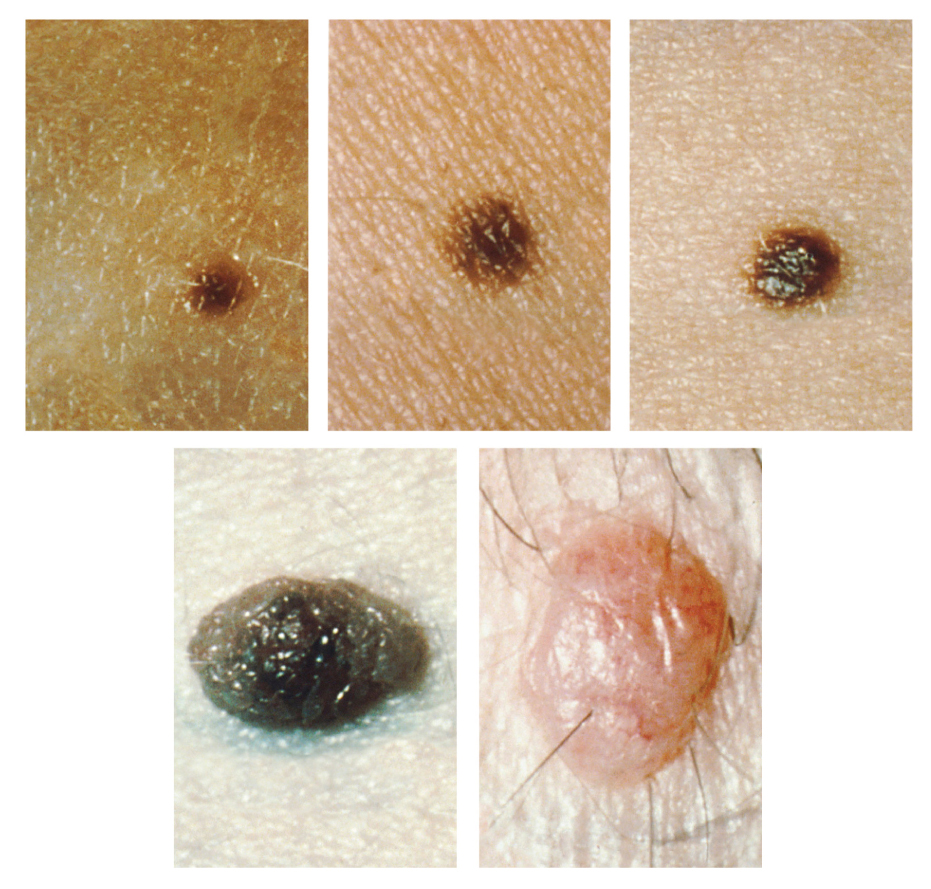
Too much sun exposure can eventually lead to wrinkling due to the destruction of the cellular structure of the skin, and in severe cases, can cause sufficient DNA damage to result in skin cancer. When there is an irregular accumulation of melanocytes in the skin, freckles appear. Moles are larger masses of melanocytes, and although most are benign, they should be monitored for changes that might indicate the presence of cancer (Figure 5.1.8). A total lack of melanin is caused by the genetic disorder called albinism (See Disorders of the…Integumentary System below)
Albinism is a genetic disorder that affects (completely or partially) the coloring of skin, hair, and eyes. The defect is primarily due to the inability of melanocytes to produce melanin. Individuals with albinism tend to appear white or very pale due to the lack of melanin in their skin and hair. Recall that melanin helps protect the skin from the harmful effects of UV radiation. Individuals with albinism tend to need more protection from UV radiation, as they are more prone to sunburns and skin cancer. They also tend to be more sensitive to light and have vision problems due to the lack of pigmentation on the retinal wall. Treatment of this disorder usually involves addressing the symptoms, such as limiting UV light exposure to the skin and eyes. In vitiligo, the melanocytes in certain areas lose their ability to produce melanin, possibly due to an autoimmune reaction. This leads to a loss of color in patches (Figure 5.1.9). Neither albinism nor vitiligo directly affects the lifespan of an individual.

Other changes in the appearance of skin coloration can be indicative of diseases associated with other body systems. Liver disease or liver cancer can cause the accumulation of bile and the yellow pigment bilirubin, leading to the skin appearing yellow or jaundiced (jaune is the French word for “yellow”). Tumors of the pituitary gland can result in the secretion of large amounts of melanocyte-stimulating hormone (MSH), which results in a darkening of the skin. Similarly, Addison’s disease can stimulate the release of excess amounts of adrenocorticotropic hormone (ACTH), which can give the skin a deep bronze color. A sudden drop in oxygenation can affect skin color, causing the skin to initially turn ashen (white). With a prolonged reduction in oxygen levels, dark red deoxyhemoglobin becomes dominant in the blood, making the skin appear blue, a condition referred to as cyanosis (kyanos is the Greek word for “blue”). This happens when the oxygen supply is restricted, as when someone is experiencing difficulty in breathing because of asthma or a heart attack. However, in these cases the effect on skin color has nothing do with the skin’s pigmentation.
External Website

This ABC video follows the story of a pair of fraternal African-American twins, one of whom is albino. Watch this video to learn about the challenges these children and their family face. Which ethnicities do you think are exempt from the possibility of albinism?
Chapter Review
The skin is composed of two major layers: a superficial epidermis and a deeper dermis. The epidermis consists of several layers beginning with the innermost (deepest) stratum basale (germinatum), followed by the stratum spinosum, stratum granulosum, stratum lucidum (when present), and ending with the outermost layer, the stratum corneum. The topmost layer, the stratum corneum, consists of dead cells that shed periodically and is progressively replaced by cells formed from the basal layer. The stratum basale also contains melanocytes, cells that produce melanin, the pigment primarily responsible for giving skin its color. Melanin is transferred to keratinocytes in the stratum spinosum to protect cells from UV rays.
The dermis connects the epidermis to the hypodermis, and provides strength and elasticity due to the presence of collagen and elastin fibers. It has only two layers: the papillary layer with papillae that extend into the epidermis and the lower, reticular layer composed of loose connective tissue. The hypodermis, deep to the dermis of skin, is the connective tissue that connects the dermis to underlying structures; it also harbors adipose tissue for fat storage and protection.
Interactive Link Questions
The skin consists of two layers and a closely associated layer. View this animation to learn more about layers of the skin. What are the basic functions of each of these layers?
The epidermis provides protection, the dermis provides support and flexibility, and the hypodermis (fat layer) provides insulation and padding.
[link] If you zoom on the cells at the outermost layer of this section of skin, what do you notice about the cells?
[link] These cells do not have nuclei, so you can deduce that they are dead. They appear to be sloughing off.
[link] If you zoom on the cells of the stratum spinosum, what is distinctive about them?
[link] These cells have desmosomes, which give the cells their spiny appearance.
This ABC video follows the story of a pair of fraternal African-American twins, one of whom is albino. Watch this video to learn about the challenges these children and their family face. Which ethnicities do you think are exempt from the possibility of albinism?
There are none.
Review Questions
Critical Thinking Questions
1. What determines the color of skin, and what is the process that darkens skin when it is exposed to UV light?
Glossary
- albinism
- genetic disorder that affects the skin, in which there is no melanin production
- basal cell
- type of stem cell found in the stratum basale and in the hair matrix that continually undergoes cell division, producing the keratinocytes of the epidermis
- dermal papilla
- (plural = dermal papillae) extension of the papillary layer of the dermis that increases surface contact between the epidermis and dermis
- dermis
- layer of skin between the epidermis and hypodermis, composed mainly of connective tissue and containing blood vessels, hair follicles, sweat glands, and other structures
- desmosome
- structure that forms an impermeable junction between cells
- elastin fibers
- fibers made of the protein elastin that increase the elasticity of the dermis
- eleiden
- clear protein-bound lipid found in the stratum lucidum that is derived from keratohyalin and helps to prevent water loss
- epidermis
- outermost tissue layer of the skin
- hypodermis
- connective tissue connecting the integument to the underlying bone and muscle
- integumentary system
- skin and its accessory structures
- keratin
- type of structural protein that gives skin, hair, and nails its hard, water-resistant properties
- keratinocyte
- cell that produces keratin and is the most predominant type of cell found in the epidermis
- keratohyalin
- granulated protein found in the stratum granulosum
- Langerhans cell
- specialized dendritic cell found in the stratum spinosum that functions as a macrophage
- melanin
- pigment that determines the color of hair and skin
- melanocyte
- cell found in the stratum basale of the epidermis that produces the pigment melanin
- melanosome
- intercellular vesicle that transfers melanin from melanocytes into keratinocytes of the epidermis
- Merkel cell
- receptor cell in the stratum basale of the epidermis that responds to the sense of touch
- papillary layer
- superficial layer of the dermis, made of loose, areolar connective tissue
- reticular layer
- deeper layer of the dermis; it has a reticulated appearance due to the presence of abundant collagen and elastin fibers
- stratum basale
- deepest layer of the epidermis, made of epidermal stem cells
- stratum corneum
- most superficial layer of the epidermis
- stratum granulosum
- layer of the epidermis superficial to the stratum spinosum
- stratum lucidum
- layer of the epidermis between the stratum granulosum and stratum corneum, found only in thick skin covering the palms, soles of the feet, and digits
- stratum spinosum
- layer of the epidermis superficial to the stratum basale, characterized by the presence of desmosomes
- vitiligo
- skin condition in which melanocytes in certain areas lose the ability to produce melanin, possibly due an autoimmune reaction that leads to loss of color in patches
Solutions
Answers for Critical Thinking Questions
- The pigment melanin, produced by melanocytes, is primarily responsible for skin color. Melanin comes in different shades of brown and black. Individuals with darker skin have darker, more abundant melanin, whereas fair-skinned individuals have a lighter shade of skin and less melanin. Exposure to UV irradiation stimulates the melanocytes to produce and secrete more melanin.
This work, Anatomy & Physiology, is adapted from Anatomy & Physiology by OpenStax, licensed under CC BY. This edition, with revised content and artwork, is licensed under CC BY-SA except where otherwise noted.
Images, from Anatomy & Physiology by OpenStax, are licensed under CC BY except where otherwise noted.
Access the original for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction.
