58 Psychopathy
Original chapter by Chris Patrick adapted by the Queen’s University Psychology Department
This Open Access chapter was originally written for the NOBA project. Information on the NOBA project can be found below.
Psychopathy (or “psychopathic personality”) is a topic that has long fascinated the public at large as well as scientists and clinical practitioners. However, it has also been subject to considerable confusion and scholarly debate over the years. This module reviews alternative conceptions of psychopathy that have been proposed historically, and reviews major instruments currently in use for the assessment of psychopathic tendencies in clinical and nonclinical samples. An integrative theoretic framework, the Triarchic model, is presented that provides a basis for reconciling differing historic conceptions and assessment approaches. Implications of the model for thinking about causal hypotheses of psychopathy, and for resolving longstanding points of contention in the field, are discussed.
Learning Objectives
- Learn about Cleckley’s classic account of psychopathy, presented in his book The Mask of Sanity, along with other historic conceptions.
- Compare and contrast differing inventories currently in use for assessing psychopathy in differing samples (e.g., adults and younger individuals, within clinical-forensic and community settings).
- Become familiar with the Triarchic model of psychopathy and its constituent constructs of boldness, meanness, and disinhibition.
- Learn about alternative theories regarding the causal origins of psychopathy.
- Consider how longstanding matters of debate regarding the nature, definition, and origins of psychopathy can be addressed from the perspective of the Triarchic model.
Introduction

For many in the public at large, the term “psychopath” conjures up images of ruthless homicidal maniacs and criminal masterminds. This impression is reinforced on an ongoing basis by depictions of psychopathic individuals in popular books and films, such as No Country for Old Men, Silence of the Lambs, and Catch Me if You Can, and by media accounts of high-profile criminals ranging from Charles Manson to Jeffrey Dahmer to Bernie Madoff. However, the concept of psychopathy(“psychopathic personality”) held by experts in the mental health field differs sharply from this common public perception—emphasizing distinct dispositional tendencies as opposed to serious criminal acts of one sort or another. This module reviews historic and contemporary conceptions of psychopathy as a clinical disorder, describes methods for assessing it, and discusses how a new conceptual model can help to address key questions regarding its nature and origins that have long been debated. It will be seen from this review that the topic remains no less fascinating or socially relevant when considered from a clinical–scientific perspective.
Historic Conceptions
Early writers characterized psychopathy as an atypical form of mental illness in which rational faculties appeared normal but everyday behavior and social relationships are markedly disrupted. French physician Philippe Pinel (1806/1962) documented cases of what he called manie sans delire (“insanity without delirium”), in which dramatic episodes of recklessness and aggression occurred in individuals not suffering from obvious clouding of the mind. German psychiatrist Julius Koch (1888) introduced the disease-oriented term psychopathic to convey the idea that conditions of this type had a strong constitutional-heritable basis. In his seminal book The Mask of Sanity, which focused on patients committed for hospital treatment, American psychiatrist Hervey Cleckley (1941/1976) described psychopathy as a deep-rooted emotional pathology concealed by an outward appearance of good mental health. In contrast with other psychiatric patients, psychopathic individuals present as confident, sociable, and well adjusted. However, their underlying disorder reveals itself over time through their actions and attitudes. To facilitate identification of psychopathic individuals in clinical settings, Cleckley provided 16 diagnostic criteria distilled from his clinical case summaries, encompassing indicators of apparent psychological stability (e.g., charm and intelligence, absence of nervousness) along with symptoms of behavioral deviancy (e.g., irresponsibility, failure to plan) and impaired affect and social connectedness (e.g., absence of remorse, deceptiveness, inability to love).

Notably, Cleckley did not characterize psychopathic patients as inherently cruel, violent, or dangerous. Although some engaged in repetitive violent acts, more often the harm they caused was nonphysical and the product of impulsive self-centeredness as opposed to viciousness. Indeed, Cleckley’s case histories included examples of “successful psychopaths” who ascended to careers as professors, medical doctors, or businessmen, along with examples of more aimless dysfunctional types. In contrast with this, other writers from Cleckley’s time who were concerned with criminal expressions of psychopathy placed greater emphasis on symptoms of emotional coldness, aggression, and predatory victimization. For example, McCord and McCord (1964) described the condition in more generally pathologic terms, highlighting “guiltlessness” (lack of remorse) and “lovelessness” (lack of attachment capacity) as central defining features.
Cleckley’s conception served as a referent for the diagnosis of psychopathy in the first two editions of the official American psychiatric nosology, the Diagnostic and Statistical Manual of Mental Disorders (DSM). However, a dramatic shift occurred in the third edition of the DSM, with the introduction of behaviorally oriented symptom definitions for most disorders to address longstanding problems of reliability. The Cleckley-oriented conception of psychopathy in prior editions was replaced by antisocial personality disorder (ASPD), defined by specific indicants of behavioral deviancy in childhood (e.g., fighting, lying, stealing, truancy) continuing into adulthood (manifested as repeated rulebreaking, impulsiveness, irresponsibility, aggressiveness, etc.). Concerns with this new conception were expressed by psychopathy experts, who noted that ASPD provided limited coverage of interpersonal-affective symptoms considered essential to psychopathy (e.g., charm, deceitfulness, selfishness, shallow affect; Hare, 1983). Nonetheless, ASPD was retained in much the same form in the fourth edition of the DSM (DSM-IV; American Psychiatric Association [APA, 2000]), and remained unchanged in the fifth edition of the DSM (American Psychiatric Association, 2013). That said, the DSM-5 does include a new, dimensional-trait approach to characterizing personality pathology (Strickland, Drislane, Lucy, Krueger, & Patrick, in press).
Contemporary assessment methods
Modern approaches to the assessment of psychopathy, consisting of rating instruments and self-report scales, reflect the foregoing historic conceptions to differing degrees.
Psychopathy in adult criminal offenders
The most widely used instrument for diagnosing psychopathy in correctional and forensic settings is the Psychopathy Checklist-Revised (PCL-R; Hare, 2003), which comprises 20 items rated on the basis of interview and file-record information. The items of the PCL-R effectively capture the interpersonal-affective deficits and behavioral deviance features identified by Cleckley, but include only limited, indirect coverage of positive adjustment features. The manual for the PCL-R recommends the use of a cutoff score of 30 out of 40 for assigning a diagnosis of psychopathy. High overall PCL-R scores are correlated with impulsive and aggressive tendencies, low empathy, Machiavellianism, lack of social connectedness, and persistent violent offending. Given these correlates, and the omission of positive adjustment indicators, psychopathy as assessed by the PCL-R appears more similar to the predatory-aggressive conception of McCord and McCord than to Cleckley’s conception.
Although the PCL-R was developed to index psychopathy as a unitary condition, structural analyses of its items reveal distinct interpersonal-affective and antisocial deviance subdimensions (factors). Although moderately (about .5) correlated, these factors show contrasting relations with external criterion measures. The interpersonal-affective factor relates to indices of narcissism, low empathy, and proactive aggression (Hare, 2003), and to some extent (after controlling for its overlap with the antisocial factor) adaptive tendencies such as high social assertiveness and low fear, distress, and depression (Hicks & Patrick, 2006). High scores on the antisocial deviance factor, by contrast, are associated mainly with maladaptive tendencies and behaviors, including impulsiveness, sensation seeking, alienation and mistrust, reactive aggression, early and persistent antisocial deviance, and substance-related problems.
Psychopathy in noncriminal adults

Psychopathy has most typically been assessed in noncriminal adult samples using self-report-based measures. Older measures of this type emphasized the antisocial deviancy component of psychopathy with limited coverage of interpersonal-affective features (Hare, 2003). Some newer instruments provide more balanced coverage of both. One example is the now widely used Psychopathic Personality Inventory (PPI; Lilienfeld & Andrews, 1996), which was developed to index personality dispositions embodied within historic conceptions of psychopathy. Its current revised form (PPI-R; Lilienfeld & Widows, 2005) contains 154 items, organized into eight facet scales.
Like the items of the PCL-R, the subscales of the PPI cohere around two distinguishable factors: a fearless dominance (FD) factor reflecting social potency, stress immunity, and fearlessness, and a self-centered impulsivity (SCI) factor reflecting egocentricity, exploitativeness, hostile rebelliousness, and lack of planning. However, unlike the factors of the PCL-R, the two PPI factors are uncorrelated, and thus even more distinct in their external correlates. Scores on PPI-FD are associated with indices of positive psychological adjustment (e.g., higher well-being; lower anxiety and depression) and measures of narcissism (low) empathy, and thrill/adventure seeking (Benning, Patrick, Blonigen, Hicks, & Iacono, 2005). Given this, PPI-FD has been interpreted as capturing a more adaptive expression of dispositional fearlessness (i.e., boldness; see below) than the interpersonal-affective factor of the PCL-R—which can be viewed as tapping a more pathologic (antagonistic or “mean”) expression of fearlessness. Scores on PPI-SCI, like Factor 2 of the PCL-R, are associated with multiple indicators of deviancy—including impulsivity and aggressiveness, child and adult antisocial behavior, substance abuse problems, heightened distress and dysphoria, and suicidal ideation.
Psychopathy in child and adolescent clinical samples
Different inventories exist for assessing psychopathic tendencies in children and adolescents. The best-known consist of rating-based measures developed, using the PCL-R as a referent, to identify psychopathic individuals among youth convicted of crimes or referred for treatment of conduct problems. The emphasis in work of this type has been on the importance of psychopathic features for predicting greater severity and persistence of conduct problems. Termed “callous-unemotional” traits, these features encompass low empathy, deficient remorse or guilt, shallow affect, and lack of concern about performance in school and other contexts (Frick & Moffitt, 2010).
One extensively researched measure for assessing psychopathic tendencies in youth is the Antisocial Process Screening Device (APSD; Frick & Marsee, 2006), used with clinic-referred children ages 6 through 13. The APSD includes 20 items completed by parents or teachers. As with the PCL-R and PPI, the items of the APSD tap two distinct factors: a Callous-Unemotional (CU) traits factor, reflecting emotional insensitivity and disregard for others; and an Impulsive/Conduct Problems (I/CP) factor, reflecting impulsivity, behavioral deviancy, and inflated self-importance. Children high on the I/CP factor alone show below-average intelligence, heightened emotional responsiveness to stressors, and angry (reactive) aggression (Frick & Marsee, 2006). By contrast, children high on both APSD factors show average or above-average intelligence, low reported levels of anxiety and nervousness, reduced reactivity to stressful events, and preference for activities entailing novelty and risk. They also learn less readily from punishment and engage in high levels of premeditated as well as reactive aggression and exhibit more persistent violent behavior across time. Given the documented importance of CU traits in moderating the expression of conduct disorder, the upcoming fifth edition of the DSM will include criteria for designating a distinct CU variant of child conduct disorder (Frick & Moffitt, 2010).
Core ingredients of psychopathy: disinhibition, boldness, and meanness
The foregoing material highlights the fact that historic conceptions of psychopathy and available instruments for assessing it place differing emphasis on different symptomatic features. This had contributed to longstanding disagreements among scholars about what psychopathy entails and what causes it. A theoretic conceptualization formulated recently to reconcile alternative perspectives is the Triarchic model (Patrick, Fowles, & Krueger, 2009). This model conceives of psychopathy as encompassing three separable symptomatic components—disinhibition, boldness, and meanness—that can be viewed as thematic building blocks for differing conceptions of psychopathy.
Definitions

Disinhibition as described in the Triarchic model encompasses tendencies toward impulsiveness, weak behavioral restraint, hostility and mistrust, and difficulties in regulating emotion. Meanness entails deficient empathy, lack of affiliative capacity, contempt toward others, predatory exploitativeness, and empowerment through cruelty and destructiveness. Referents for disinhibition and meanness include the finding of distinct I/CP and CU factors in the child psychopathy literature and corresponding evidence for distinct disinhibitory and callous-aggression factors underlying impulse control (externalizing) problems in adults (Krueger, Markon, Patrick, Benning, & Kramer, 2007). The third construct in the model, Boldness,encompasses dominance, social assurance, emotional resiliency, and venturesomeness. Referents for this construct include the “mask” elements of Cleckley’s conception, Lykken’s (1995) low fear theory of psychopathy, the FD factor of the PPI, and developmental research on fearless temperament as a possible precursor to psychopathy (Patrick et al., 2009).
From the perspective of the Triarchic model, Cleckley’s conception of psychopathy emphasized boldness and disinhibition, whereas criminally oriented conceptions (and affiliated measures, including the PCL-R and APSD) emphasize meanness and disinhibition more so. According to the model, individuals high in disinhibitory tendencies would warrant a diagnosis of psychopathy if also high in boldness or meanness (or both), but individuals high on only one of these tendencies would not. Individuals with differing relative elevations on these three symptomatic components would account for contrasting variants (subtypes) of psychopathy as described in the literature (Hicks, Markon, Patrick, Krueger, & Newman, 2004; Karpman, 1941; Skeem, Johansson, Andershed, Kerr, & Louden, 2007).
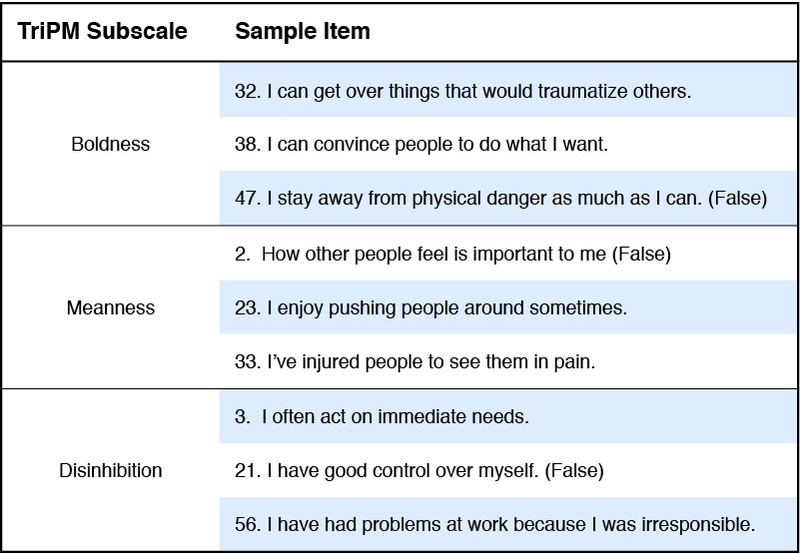
An inventory designed specifically to operationalize this model is the Triarchic Psychopathy Measure (TriPM; Patrick, 2010). The TriPM contains 58 items comprising three subscales that correspond to the constructs of the model (see Table 1). The items of the Disinhibition and Meanness scales (20 and 19 items, respectively) are taken from the Externalizing Spectrum Inventory (ESI; Krueger et al., 2007), a measure of problems and traits associated with externalizing psychopathology. The TriPM Boldness scale was developed to index fearless tendencies in social, affective-experiential, and activity preference domains, with reference to the FD factor of the PPI and the general factor shown to underlie differing scale measures of fear and fearlessness (Kramer, Patrick, Gasperi, & Krueger, 2012).
Although the TriPM is relatively new, promising evidence for its convergent and discriminant validity has begun to appear (e.g., Sellbom & Phillips, 2013; Strickland et al., in press; see also Venables & Patrick, 2012). Given that the inventory is freely available online, and that several foreign-language translations now exist (including Brazilian-Portuguese, Dutch, Finnish, German, Italian, Portuguese, Swedish, and Spanish), it can be expected that additional validity data will accumulate rapidly over time. Work is also being done to evaluate whether effective scale measures of the Triarchic constructs can be derived from items of other existing psychopathy inventories such as the PPI. As discussed in the last part of this section, research examining the common and distinctive correlates of these three components of psychopathy is likely to be helpful for addressing and perhaps resolving ongoing points of uncertainty and debate in the field.
Causal factors
Considerable research has been devoted over many years to investigation of causal factors in psychopathy. Existing theories are of two types: (1) theories emphasizing core deficits in emotional sensitivity or responsiveness, and (2) theories positing basic impairments in cognitive-attentional processing (Patrick & Bernat, 2009). In support of these alternative theories, differing neurobiological correlates of psychopathy have been reported. One of the most consistent entails a lack of normal enhancement of the startle blink reflex to abrupt noises occurring during viewing of aversive foreground stimuli (e.g., scary or disturbing pictorial images) as compared with neutral or pleasant stimuli (see Figure 1). This result, akin to a failure to “jump” upon hearing a trash can tip while walking alone in a dark alley, has been interpreted as reflecting a lack of normal defensive (fear) reactivity. Another fairly consistent finding involves reduced amplitude of brain potential response to intermittent target stimuli, or following incorrect responses, within cognitive performance tasks—indicative of reduced cortical-attentional processing or impaired action monitoring (Patrick & Bernat, 2009). Yet other research using functional neuroimaging has demonstrated deficits in basic subcortical (amygdala) reactivity to interpersonal distress cues (e.g., fearful human faces) in high-psychopathic individuals (Jones, Laurens, Herba, Barker, & Viding, 2009; Marsh et al., 2008).
The Triarchic model may prove to be of use for reconciling alternative causal models of psychopathy that have been proposed based on contrasting neurobiological and behavioral findings. For example, lack of startle enhancement during aversive cuing has been tied specifically to the interpersonal-affective factor of the PCL-R and the counterpart FD factor of the PPI (Figure 1)—suggesting a link to the boldness component of psychopathy. By contrast, reduced brain potential responses in cognitive tasks appear more related to impulsive-externalizing tendencies associated with the disinhibition component of psychopathy (Carlson, Thái, & McLaron, 2009; Patrick & Bernat, 2009). On the other hand, the finding of reduced subcortical response to affective facial cues has been tied to the CU traits factor of child/adolescent psychopathy, a referent for meanness in the Triarchic model. However, further research is needed to determine whether this finding reflects fear deficits common to meanness and boldness, or deficits in affiliative capacity or empathy specific to meanness.
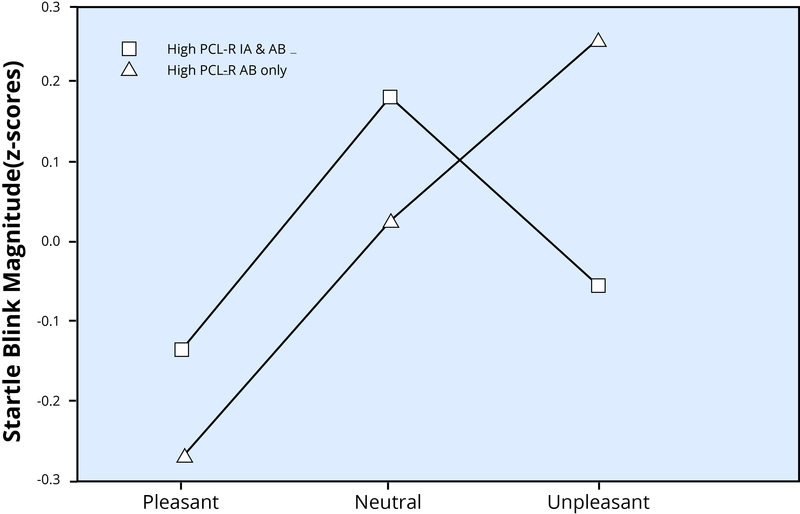
Upper plot: Mean magnitude of startle blink responses to noise probes occurring during viewing of pleasant, neutral, and unpleasant picture stimuli in two male prisoner groups: (1) prisoners scoring high on the antisocial behavior (AB) factor of the Psychopathy Checklist-Revised (PCL-R; Hare, 2003) but not the interpersonal-affective (IA) factor (labeled “High PCL-R AB only” in the plot; n = 18), and (2) prisoners high on both factors of the PCL-R (labeled “High PCL-R IA & AB”; n = 17).
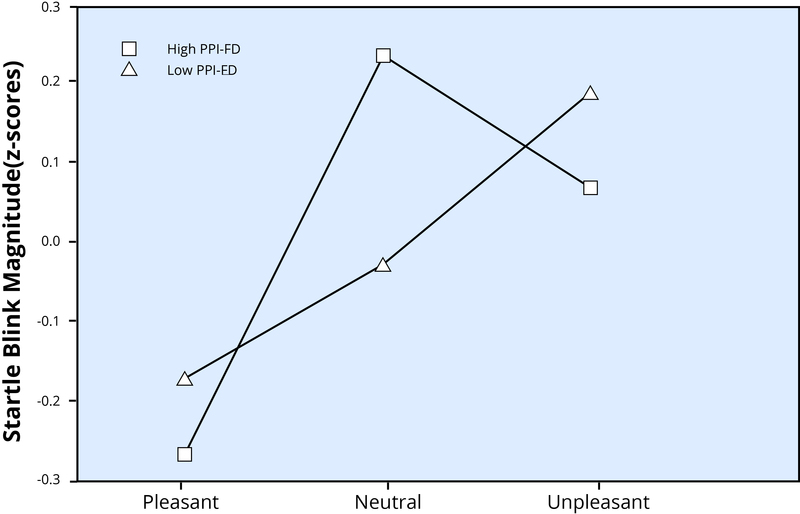
In both plots, blink means for each picture type are presented in z-score units (M = 0, SD = 1) derived by standardizing raw blink magnitude scores across trials for each individual subject. Data in the upper plot are from Patrick, Bradley, and Lang (1993); data in the lower plot are from Benning, Patrick, and Iacono (2005).
Triarchic model perspective on long-debated issues regarding psychopathy
As highlighted in the foregoing sections, scholars have grappled with issues of definition since psychopathy was first identified as a condition of clinical concern, and questions regarding its essential features and alternative expressions continue to be debated and studied. This final subsection discusses how some of the major issues of debate are addressed by the Triarchic model.
One key issue is whether psychological/emotional stability is characteristic or not of psychopathy. Cleckley’s (1941/1976) view was that psychopathy entails a salient presentation of good mental health, and his diagnostic criteria included indicators of positive adjustment. By contrast, the dominant clinical assessment devices for psychopathy, the PCL-R and ASPD, are heavily oriented toward deviancy and include no items that are purely indicative of adjustment. From a Triarchic model standpoint, the more adaptive elements of psychopathy are embodied in its boldness facet, which entails social poise, emotional stability, and enjoyment of novelty and adventure. At the same time, high boldness is also associated with narcissistic tendencies, reduced sensitivity to the feelings of others, and risk-taking (Benning et al., 2005). Thus, the concept of boldness provides a way to think about the intriguing “mask” element of psychopathy.
Related to this, another issue is whether lack of anxiety is central to psychopathy, as Cleckley and others (e.g., Fowles & Dindo, 2009; Lykken, 1995) have emphasized. This perspective is challenged by research showing either negligible or somewhat positive associations for overall scores on the PCL-R and other psychopathy measures with anxiety. The Triarchic model helps to address this inconsistency by separating the disorder into subcomponents or facets, which relate differently to measures of trait anxiety: Boldness is correlated negatively with anxiousness (Benning et al., 2005), whereas Disinhibition and Meannness are correlated negatively and negligibly, respectively, with anxiety (Venables & Patrick, 2012). Related to this, cluster analytic studies of criminal offenders exhibiting high overall scores on the PCL-R have demonstrated one subtype characterized by low anxiety in particular, and another exhibiting high anxiety along with very high levels of impulsivity and aggression (Hicks et al., 2004; Skeem et al., 2007). The implication is that low anxiousness is central to one variant of criminal psychopathy (the bold-disinhibited, or “primary” type) but not to another variant (the “disinhibited-mean,” “aggressive-externalizing,” or “secondary” type).
A further key question is whether violent/aggressive tendencies are typical of psychopathic individuals and should be included in the definition of the disorder. Cleckley’s (1941/1976) view was that “such tendencies should be regarded as the exception rather than as the rule” (p. 262). However, aggressiveness is central to criminally oriented conceptions of psychopathy, and the PCL-R includes an item reflecting hot-temperedness and aggression (“poor behavioral controls”) along with other items scored in part based on indications of cruelty and violence. In the Triarchic model, tendencies toward aggression are represented in both the disinhibition and meanness constructs, and a “mean-disinhibited” type of psychopath clearly exists, marked by the presence of salient aggressive behavior (Frick & Marsee, 2006; Hicks et al., 2004). Thus, Cleckley’s idea of aggression as ancillary to psychopathy may apply more to a variant of psychopathy that entails high boldness in conjunction with high disinhibition (Hicks et al., 2004).
Another question is whether criminal or antisocial behavior more broadly represents a defining feature of psychopathy, or a secondary manifestation (Cooke, Michie, Hart, & Clark, 2004). From the standpoint of the Triarchic model, antisocial behavior arises from the complex interplay of different “deviance-promoting” influences—including dispositional boldness, meanness, and disinhibition. However, whether approaches can be developed for classifying antisocial behaviors in ways that relate more selectively to these and other distinct influences (e.g., through reference to underlying motives, spontaneity versus premeditation) is an important topic to be addressed in future research.
Another key question is whether differing subtypes of psychopathy exist. From the perspective of the Triarchic model, alternative variants of psychopathy reflect differing configurations of boldness, meanness, and disinhibition. Viewed this way, designations such as “bold-disinhibited” and “mean-disinhibited” may prove more useful for research and clinical purposes than labels like “primary” versus “secondary” or “low anxious” versus “high anxious.” An issue from this perspective is whether individuals who are high in boldness and/or meanness but low in disinhibition would qualify for a diagnosis of psychopathy. For example, should a high-bold/high-mean individual (e.g., a ruthless corporate executive, like the one portrayed by actor Michael Douglas in the film Wall Street; Pressman & Stone, 1987)—or an extremely mean/vicious but neither bold nor pervasively disinhibited individual, such as Russian serial murder Andrei Chikatilo (Cullen, 1993)—be considered psychopathic? Questions of this sort will need to be addressed through elaborations of existing theories in conjunction with further systematic research.
Yet another question is whether psychopathy differs in women as compared to men. Cleckley’s descriptive accounts of psychopathic patients included two female case examples along with multiple male cases, and his view was that psychopathy clearly exists in women and reflects the same core deficit (i.e., absence of “major emotional accompaniments” of experience) as in men. However, men exhibit criminal deviance and ASPD at much higher rates than women (APA, 2000) and men in the population at large score higher in general on measures of psychopathy than women (Hare, 2003; Lilienfeld & Widows, 2005). From a Triarchic model perspective, these differences in prevalence may be attributable largely to differences between women and men in average levels of boldness, meanness, and disinhibition. Some supportive evidence exists for this hypothesis (e.g., findings of Hicks et al. [pb_glossary id="2006"]2007[/pb_glossary] demonstrating mediation of gender differences in ASPD symptoms by levels of externalizing proneness). Beyond this, it is important also to consider whether underlying psychopathic dispositions in men and women may be manifested differently in overt behavior (Verona & Vitale, 2006). Some intriguing evidence exists for this—including twin research findings demonstrating a genetic association between dispositional boldness (as indexed by estimated scores on PPI-FD) and a composite index of externalizing problems in male but not female participants (Blonigen, Hicks, Patrick, Krueger, Iacono, & McGue, 2005). However, more extensive research along these lines, examining all facets of the Triarchic model in relation to behavioral outcomes of differing kinds, will be required to effectively address the question of gender-moderated expression.

A final intriguing question is whether “successful” psychopaths exist. Hall and Benning (2006) hypothesized that successful psychopathy entails a preponderance of certain causal influences (resulting in particular symptomatic features) over others. Drawing on known correlates of PPI-FD (e.g., Benning et al., 2005; Ross, Benning, Patrick, Thompson, & Thurston, 2009) and theories positing separate etiologic mechanisms for differing features of psychopathy (Fowles & Dindo, 2009; Patrick & Bernat, 2009), these authors proposed that the presence of dispositional fearlessness (boldness) may be conducive to success when not accompanied by high externalizing proneness (disinhibition). For example, high-bold/low-disinhibited individuals could be expected to achieve higher success in occupations calling for leadership and/or courage because their psychopathic tendencies are manifested mainly in terms of social effectiveness, affective resilience, and venturesomeness.
Data relevant to this idea come from an intriguing study by Lilienfeld, Waldman, Landfield, Rubenzer, and Faschingbauer (2012), who used personality trait ratings of former U.S. presidents provided by expert historians to estimate scores on the FD and SCI factors of the PPI (Ross et al., 2009). They found that higher estimated levels of PPI-FD (boldness) predicted higher ratings of presidential performance, persuasiveness, leadership, and crisis management ability, whereas higher estimated levels of SCI predicted adverse outcomes such as documented abuses of power and impeachment proceedings. Further research on outcomes associated with high levels of boldness and/or meanness in the absence of high disinhibition should yield valuable new insights into dispositional factors underlying psychopathy and alternative ways psychopathic tendencies can be expressed.
Check Your Knowledge
To help you with your studying, we’ve included some practice questions for this module. These questions do not necessarily address all content in this module. They are intended as practice, and you are responsible for all of the content in this module even if there is no associated practice question. To promote deeper engagement with the material, we encourage you to create some questions of your own for your practice. You can then also return to these self-generated questions later in the course to test yourself.
Vocabulary
- Counterpart diagnosis to psychopathy included in the third through fifth editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM; APA, 2000). Defined by specific symptoms of behavioral deviancy in childhood (e.g., fighting, lying, stealing, truancy) continuing into adulthood (manifested as repeated rule-breaking, impulsiveness, irresponsibility, aggressiveness, etc.).
- Psychopathy
- Synonymous with psychopathic personality, the term used by Cleckley (1941/1976), and adapted from the term psychopathic introduced by German psychiatrist Julius Koch (1888) to designate mental disorders presumed to be heritable.
- Triarchic model
- Model formulated to reconcile alternative historic conceptions of psychopathy and differing methods for assessing it. Conceives of psychopathy as encompassing three symptomatic components: boldness, involving social efficacy, emotional resiliency, and venturesomeness; meanness, entailing lack of empathy/emotional-sensitivity and exploitative behavior toward others; and disinhibition, entailing deficient behavioral restraint and lack of control over urges/emotional reactions.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5.Washington, D.C: American Psychiatric Association.
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, DC: Author.
- Benning, S. D., Patrick, C. J., & Iacono, W. G. (2005). Psychopathy, startle blink modulation, and electrodermal reactivity in twin men. Psychophysiology, 42, 753-762.
- Benning, S. D., Patrick, C. J., Blonigen, D. M., Hicks, B. M., & Iacono, W. G. (2005). Estimating facets of psychopathy from normal personality traits: A step toward community-epidemiological investigations. Assessment, 12, 3–18.
- Blonigen, D. M., Hicks, B. M., Patrick, C. J., Krueger, R. F., Iacono, W. G., & McGue, M. K. (2005). Psychopathic personality traits: Heritability and genetic overlap with internalizing and externalizing psychopathology. Psychological Medicine, 35, 637–648.
- Carlson, S. R., Thái, S., & McLaron, M. E. (2009). Visual P3 amplitude and self-reported psychopathic personality traits: Frontal reduction is associated with self-centered impulsivity. Psychophysiology, 46, 100–113.
- Cleckley, H. (1976). The mask of sanity (5th ed.). St. Louis, MO: Mosby. (Original edition published in 1941)
- Cooke, D. J., Michie, C., Hart, S. D., & Clark, D. A. (2004). Reconstructing psychopathy: Clarifying the significance of antisocial and socially deviant behavior in the diagnosis of psychopathic personality disorder. Journal of Personality Disorders, 18, 337–357.
- Cullen, R. (1993). The killer department. Birmingham, UK: Orion Media.
- Fowles, D. C., & Dindo, L. (2009). Temperament and psychopathy: A dual-pathway model. Current Directions in Psychological Science, 18, 179–183.
- Frick, P. J., & Marsee, M. A. (2006). Psychopathy and developmental pathways to antisocial behavior in youth. In C. J. Patrick (Ed.), Handbook of psychopathy (pp. 353–374). New York, NY: Guilford Press.
- Frick, P. J., & Moffitt, T. E. (2010). A proposal to the DSM-V Childhood Disorders and the ADHD and Disruptive Behavior Disorders Work Groups to include a specifier to the diagnosis of conduct disorder based on the presence of callous-unemotional traits. Washington, DC: American Psychiatric Association. Retrieved from http://www.dsm5.org/Proposed Revision Attachments/Proposal for Callous and Unemotional Specifier of Conduct Disorder.pdf
- Hall, J. R., & Benning, S. D. (2006). The “successful” psychopath: Adaptive and subclinical manifestations of psychopathy in the general population. In C. J. Patrick (Ed.), Handbook of psychopathy (pp. 459–478). New York, NY: Guilford Press.
- Hare, R. D. (2003). The Hare Psychopathy Checklist (2nd ed.). Toronto, Canada: Multi-Health Systems. (Original edition published in 1991)
- Hare, R. D. (1983). Diagnosis of antisocial personality disorder in two prison populations. American Journal of Psychiatry, 140, 887–890.
- Hicks, B. M., & Patrick, C. J. (2006). Psychopathy and negative affectivity: Analyses of suppressor effects reveal distinct relations with trait anxiety, depression, fearfulness, and anger-hostility. Journal of Abnormal Psychology, 115, 276–287.
- Hicks, B. M., Blonigen, D. M., Iacono, W. G., Kramer, M., Krueger, R. F., McGue, M. K., & Patrick, C. J. (2007). Gender differences and developmental change in externalizing disorders from late adolescence to early adulthood: A longitudinal-twin study. Journal of Abnormal Psychology, 116, 433–447.
- Hicks, B. M., Markon, K. E., Patrick, C. J., Krueger, R. F., & Newman, J. P. (2004). Identifying psychopathy subtypes on the basis of personality structure. Psychological Assessment, 16, 276–288.
- Jones, A. P., Laurens, K. R., Herba, C. M., Barker, G. J., & Viding, E. (2009). Amygdala hypoactivity to fearful faces in boys with conduct problems and callous-unemotional traits. American Journal of Psychiatry, 166, 95–102.
- Karpman, B. (1941). On the need of separating psychopathy into two distinct clinical types: The symptomatic and the idiopathic. Journal of Criminal Psychopathology, 3, 112–137.
- Koch, J. L. (1888). Kurzgefasster leitfaden der psychiatrie [Short textbook of psychiatry]. Ravensburg, Germany: Maier.
- Kramer, M. D., Patrick, C. J., Krueger, R. F., & Gasperi, M. (2012). Delineating physiological defensive reactivity in the domain of self-report: Phenotypic and etiologic structure of dispositional fear. Psychological Medicine, 42, 1305–1320.
- Krueger, R. F., Markon, K. E., Patrick, C. J., Benning, S. D., & Kramer, M. (2007). Linking antisocial behavior, substance use, and personality: An integrative quantitative model of the adult externalizing spectrum. Journal of Abnormal Psychology, 116, 645–666.
- Lilienfeld, S. O., & Andrews, B. P. (1996). Development and preliminary validation of a self report measure of psychopathic personality traits in noncriminal populations. Journal of Personality Assessment, 66, 488–524.
- Lilienfeld, S. O., & Widows, M. R. (2005). Psychopathic Personality Inventory-Revised (PPI-R) professional manual. Odessa, FL: Psychological Assessment Resources.
- Lilienfeld, S. O., Waldman, I. D., Landfield, K., Rubenzer, S., & Faschingbauer, T. R. (2012). Psychopathic personality traits among U.S. presidents: Implications for job performance and leadership. Journal of Personality and Social Psychology, 103, 489–505.
- Lykken, D. T. (1995). The antisocial personalities. Hillsdale, NJ: Erlbaum.
- Marsh, A. A., Finger, E. C., Mitchell, D. G., Reid, M. E., Sims, C., Kosson, D. S., et al. (2008). Reduced amygdala response to fearful expressions in children and adolescents with callous-unemotional traits and disruptive behavior disorders. The American Journal of Psychiatry, 165, 712–720.
- McCord, W., & McCord, J. (1964). The psychopath: An essay on the criminal mind. Princeton, NJ: Van Nostrand.
- Patrick, C. J. (2010). Operationalizing the Triarchic conceptualization of psychopathy: Preliminary description of brief scales for assessment of boldness, meanness, and disinhibition. Unpublished test manual, Florida State University, Tallahassee, FL. Retrieved from https://www.phenxtoolkit.org/index.php?pageLink=browse.protocoldetails&id=121601
- Patrick, C. J., & Bernat, E. M. (2009). Neurobiology of psychopathy: A two-process theory. In: G. G. Berntson & J. T. Cacioppo (Eds.), Handbook of neuroscience for the behavioral sciences (pp. 1110–1131). New York, NY: John Wiley & Sons.
- Patrick, C. J., & Bernat, E. M. (2009). Neurobiology of psychopathy: A two-process theory. In: G. G. Berntson & J. T. Cacioppo (Eds.), Handbook of neuroscience for the behavioral sciences (pp. 1110–1131). New York, NY: John Wiley & Sons.
- Patrick, C. J., Bradley, M. M., & Lang, P. J. (1993). Emotion in the criminal psychopath: Startle reflex modulation. Journal of Abnormal Psychology, 102, 82-92.
- Patrick, C. J., Fowles, D. C., & Krueger, R. F. (2009). Triarchic conceptualization of psychopathy: Developmental origins of disinhibition, boldness, and meanness. Development and Psychopathology, 21, 913–938.
- Pinel, P. (1962). A treatise on insanity (D. Davis, translator). New York, NY: Hafner. (Original edition published in 1806)
- Pressman, E. R. (Producer), & Stone, O. (Director). (1987). Wall Street. United States: 20th Century Fox.
- Ross, S. R., Benning, S. D., Patrick, C. J., Thompson, A., & Thurston, A. (2009). Factors of the Psychopathic Personality Inventory: Criterion-related validity and relationship to the BIS/BAS and Five-Factor models of personality. Assessment, 16, 71–87.
- Sellbom, M., & Phillips, T. R. (2013). An examination of the triarchic conceptualization of psychopathy in incarcerated and non-incarcerated samples. Journal of Abnormal Psychology, 122, 208–214.
- Skeem, J. L., Johansson, P., Andershed, H., Kerr, M., & Louden, J. E. (2007). Two subtypes of psychopathic violent offenders that parallel primary and secondary variants. Journal of Abnormal Psychology, 116, 395–409.
- Strickland, C. M., Drislane, L. E., Lucy, M., Krueger, R. F., & Patrick, C. J. (in press). Characterizing psychopathy using DSM-5 personality traits. Assessment.
- Venables, N. C., & Patrick, C. J. (2012). Validity of the Externalizing Spectrum Inventory in a criminal offender sample: Relations with disinhibitory psychopathology, personality, and psychopathic features. Psychological Assessment, 24, 88–100.
- Verona, E., & Vitale, J. (2006). Psychopathy in women: Assessment, manifestations, and etiology. In C. J. Patrick (Ed.), Handbook of psychopathy (pp. 415–436). New York, NY: Guilford Press.
How to cite this Chapter using APA Style:
Patrick, C. (2019). Psychopathy. Adapted for use by Queen’s University. Original chapter in R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/ysg8mu9w
Copyright and Acknowledgment:
This material is licensed under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. To view a copy of this license, visit: http://creativecommons.org/licenses/by-nc-sa/4.0/deed.en_US.
This material is attributed to the Diener Education Fund (copyright © 2018) and can be accessed via this link: http://noba.to/ysg8mu9w.
Additional information about the Diener Education Fund (DEF) can be accessed here.