Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
6.2 Family History
Family Health History
Family health history-based risk assessment is still the gold standard in the initial assessment for heritable conditions. It is the least expensive genetic test available. The best way to identify red flags is by taking a family history (in addition to a personal health history).
A family health history records the health conditions of an individual and their biological relatives (alive and deceased), helping to identify genetic and heritable risks for certain diseases. It is often depicted through a family tree or pedigree.
Discussing genetic risk can be upsetting for some individuals. Nurses must consider the psychosocial aspects of risk assessment and use their training in relational practice and counseling during these conversations. Genetic counselors specialize in providing guidance and support to individuals and families about genetic conditions and their potential health implications. When genetic counselors are available, nurses should collaborate with them, ensuring that each professional works within their respective scope of practice. This collaborative approach ensures comprehensive care and support for patients.
Why take a family history?
All diseases have some genetic component, and the strength of the genetic component may be revealed by a family history.
Family history, alone or in combination with other risk factors, increases the risk for common diseases, (i.e. heart disease, diabetes, and various cancers) much more than genetic variants, alone or in combination, can predict.
Even with advancing genomic technology, family history is still the gold standard to assess the likelihood of a genetic condition and to identify individuals who may benefit from referral to a specialist.
Pattern of inheritance can be demonstrated by a family history.
Family history can help to make or refine a diagnosis, particularly in conditions of variable expressivity (where not all individuals present with the same symptoms of a condition). For example, in hereditary hemochromatosis, a family history could reveal diabetes, liver failure, heart disease and/or early death in multiple family members.
Family history can affect testing, treatment, surveillance and management recommendations. For example, a woman’s eligibility for the Ontario Breast Screening Program (OBSP) could be determined.
Taking the time to explore your patient’s family history is an opportunity to build rapport, provide patient education, and to correct misconceptions.
Drawing the family history in a pedigree format makes it easy to be read by other healthcare providers and easy to update.
Read
Hickey, K.T., Katapodi, M.C., Coleman, B., Reuter-Rice, K. & Starkweather, A.R. (2017). Improving utilization of the family history in the electronic health record. Journal of Nursing Scholarship, 49, 80-86. https://doi.org/10.1111/jnu.12259
When should I take a family history?
A good place to start is at your first visit with a new patient. Risk assessment is an ongoing process, so the family history should be regularly updated. Take note of the life stage of your patient as questions may vary as patients age. For example, questions relevant for a pediatric patient will be different than those for a woman of childbearing age or a man in his late sixties.
How is a family history taken?
For each individual in the family:
Ask about general health now and in earlier life
Ask about development and intellectual functioning
If deceased, ask about the age and cause
Start with your patient and ask about his/her children and his/her partner. Note:
Consanguinity (“Are you and your partner related by blood e.g. cousins?”)
Children from previous relationships
Miscarriages and terminations of pregnancy (note if for medical reason and at what gestational age)
Ask about your patient’s siblings and his/her children (nieces and nephews) and his/her partner’s siblings and their children. Note full or half siblings (“Do your brothers and sisters have the same mother and father?”). Ask about your patient’s parents and his/her partner’s parents. If your patient does not have children, ask about grandparents on both sides of the family.
A three generation pedigree is generally accepted as the standard. Once this is complete, ask in general about other relatives, have your patient think of aunts, uncles and cousins, and ask:
Are there any diseases that seem to run in the family?
Is there a history of infertility, a couple that had more than three miscarriages, or a couple that had difficulty getting pregnant? If yes, do you know the reason?
Are there any known genetic conditions in the family, for example cystic fibrosis or muscular dystrophy?
Was anyone born with a physical difference, for example a hole in the heart or extra digits, or with congenital hearing loss?
Did any children die at birth or at a young age?
Is there a history of intellectual disability or developmental delay?
Is there any cancer in the family? If so, what type and at what age?
Is there any heart disease at an early age (under age 60)?
Example – Family History Risk Assessment Questionnaire
Generally defined as a union between two individuals related as second cousins or closer
Higher than average chance for both members of a couple to be carriers of the same autosomal recessive condition
History of congenital anomalies (e.g. heart defect, imperforate anus), still birth, childhood death, infertility, more than three unexplained miscarriages
After a general, three-generation family history is obtained, if there are red flags (e.g. multiple affected relatives, young age of diagnosis, see this point of care tool for more) you can use the tools below to complete a more targeted history can help to identify those who may qualify for modified screening (e.g. starting earlier, more frequent, alternate modality), a genetic assessment and/or genetic testing.
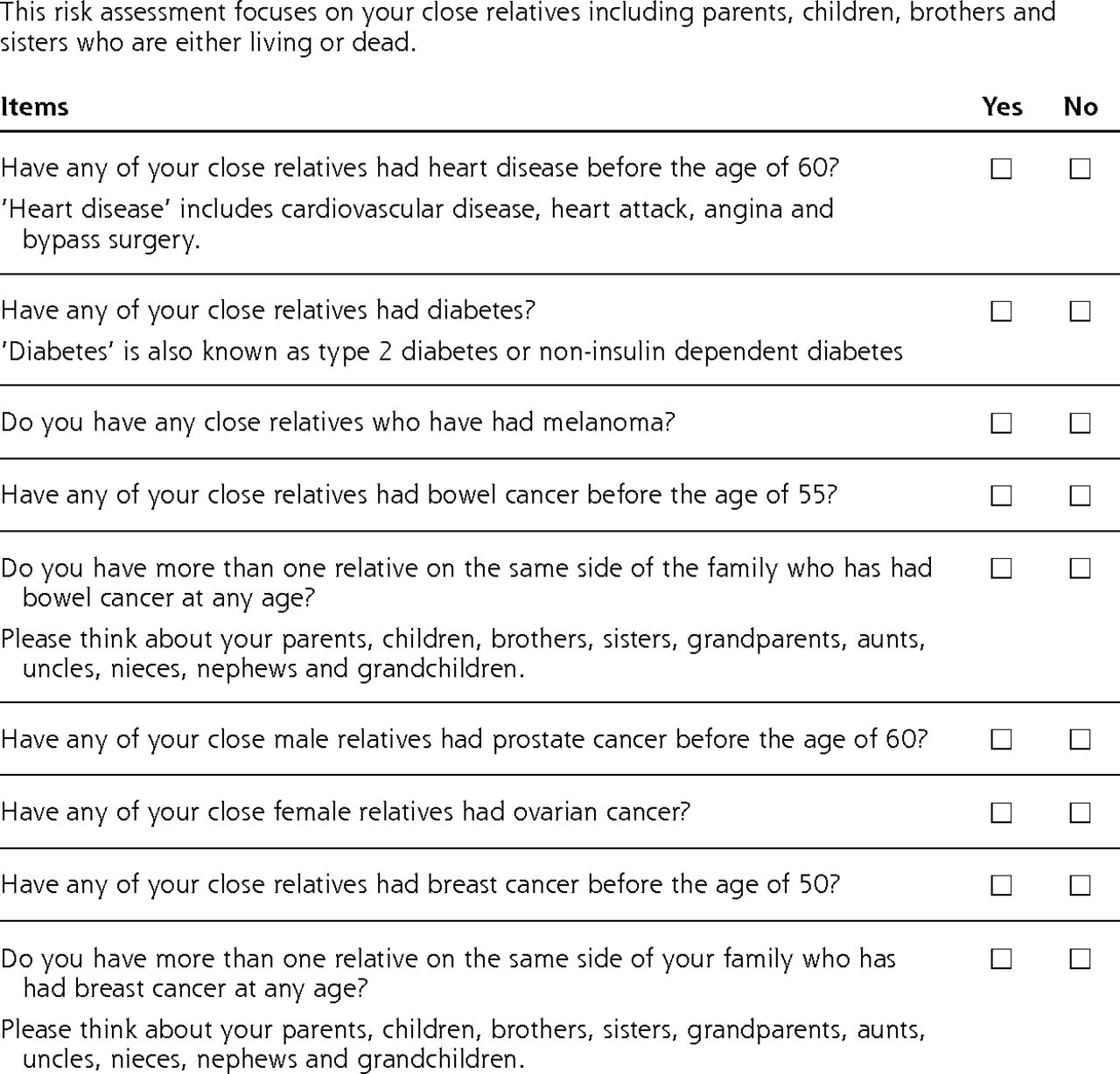
Fig 6.1 Example – Family History Risk Assessment Questionnaire
This risk assessment focuses on your close relatives including parents, children, brothers and sisters who are either living or dead.
Have any of your close relatives had heart disease before the age of 60? ‘Heart disease’ includes cardiovascular disease, heart attack, angina and bypass surgery.
Have any of your close relatives had diabetes? ‘Diabetes’ is also known as type 2 diabetes or non-insulin dependent diabetes.
Do you have any close relatives have had melanoma?
Have any of your close relatives had bowel cancer before the age of 55?
Do you have more than one relative on the same side of the family who has had bowel cancer at any age? Please think about your parents, children, brothers, sisters, grandparents, aunts, uncles, nieces, nephews and grandchildren.
Have any of your close male relatives had prostate cancer before the age of 60?
Have any of your close female relatives had ovarian cancer?
Have any of your close relatives had breast cancer before the age of 50?
Do you have more than one relative on the same side of your family who has had breast cancer at any age? Please think about your parents, children, brothers, sisters, grandparents, aunts, uncles, nieces, nephews and grandchildren. [Back to Fig 6.1]
Attribution & References
Except where otherwise noted, this content is adapted from:
Emery, J. D., Reid, G., Prevost, A. T., Ravine, D., & Walter, F. M. (2014). Development and validation of a family history screening questionnaire in Australian primary care. The Annals of Family Medicine, 12(3), 241–249. https://doi.org/10.1370/afm.1617