Oral Embryology
What is Embryology?
Embryology is the study of prenatal development from conception to birth. The interval between fertilization of the ovum (egg) by the sperm and birth is known as the gestation period. The 9-month human gestation period is divided by embryologists into three distinct developmental periods:
- The preimplantation period is the week from fertilization of the egg until implantation of the zygote on the uterine wall.
- The embryonic period lasts from the second through the eighth week of development. It contains some of the most critical changes in development, including the differentiation of organs in the embryo.
- The fetal period is the final stage of development, starting with the ninth week of gestation and lasting until birth. It is marked by the growth of the fetus and maturation of the organs and body systems in preparation for independent living outside the mother’s womb.
The Preimplantation Period
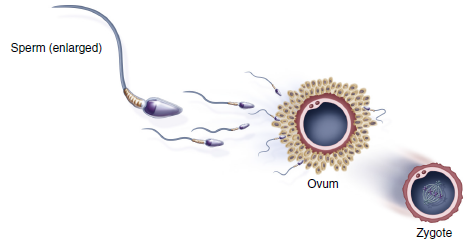
The preimplantation period begins after the male reproductive cell, the sperm, penetrates the female cell, the ovum, in a process called fertilization. The fertilized egg, called a zygote, has 46 chromosomes: 23 from the sperm cell and 23 from the ovum itself. These chromosomes will determine its inherited characteristics and will direct growth and development. The process of joining parents’ chromosomes is called meiosis.
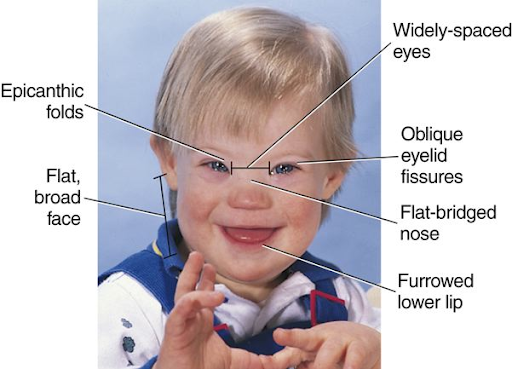
Occasionally, too many or too few chromosomes occupy the zygote as the result of a disturbance during fertilization or a defect in the sperm or egg. One such condition, called trisomy 21, results from the presence of three chromosomes 21 instead of the normal two (one from each parent). Trisomy 21, also called Down syndrome, results in varying degrees of facial changes (refer to bottom image) and intellectual disability, in addition to other physical abnormalities and defects.
 |
 |
|
Formation of the zygote |
Child with Down syndrome (Trisomy 21) |
The Embryonic Period
Perhaps the most important stage of development is the embryonic period. It is during these seven weeks that the embryo’s cells differentiate or specialize into cells with specific purposes.
The embryo is originally a ball of cells that results from the rapid division of the cells of the zygote. This ball of cells consists of three layers that can be followed all the way from their earliest beginning to maturity in the fetus.
The three layers are:
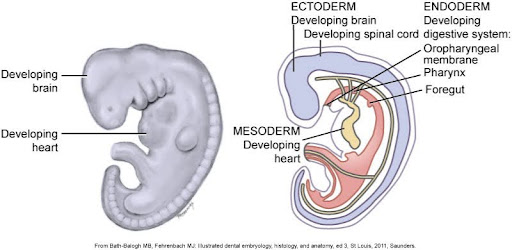
- The outer layer, or ectoderm, eventually gives rise to such structures as the skin, hair, nails, central nervous system, and tooth enamel.
- The middle layer, or mesoderm, differentiates into muscle, bone, blood, and the rest of each tooth.
- The inner core of the embryo, the endoderm, is responsible for forming the digestive system.
Any disturbance of an embryonic layer may result in abnormal growth of one or several of the structures that develop from that layer.
The diagrams below depict an embryo during early development: On the left, a side view of an embryo shows a developing brain and heart; on the right, a cross-section labeling the three embryonic layers—ectoderm, mesoderm, and endoderm—with structures like the developing brain, heart, and digestive system highlighted.
Fetal Period
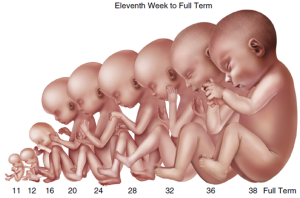
The fetal period begins in the ninth week and lasts until birth. During this period, body systems continue to develop and mature. The fetus has distinguishable ears, arms, hands, feet, legs, fingers, and footprints. Because all organ systems are formed during the embryonic stage, the fetus is less vulnerable to malformations caused by drugs, viruses, and radiation. The fetal stage is a period of growth and maturation.
Activity 1: Development Periods
Activity 2: Embryonic Layers and Structures Formed
Developmental Disturbances of the Embryonic Period
As you’ll recall, the ectoderm layer of the embryo is responsible for forming the skin, nails, hair, and tooth enamel. A genetic condition known as ectodermal dysplasia (images below on the left) exerts its effects on all of these structures, resulting in thin, pale, dry skin, abnormally shaped nails, sparse hair, and missing and malformed teeth.
Another genetic disorder, dentinogenesis imperfecta (image below on the right), affects the mesoderm, resulting in the production of faulty dentin. Dentinogenesis imperfecta is characterized by opalescent teeth that are prone to fracture because of their soft dentin. The condition is sometimes seen in children with another genetic disorder of the mesoderm, osteogenesis imperfecta, which results in weak bones.
 |
 |
|
Ectodermal dysplasia |
Dentinogenesis imperfecta |
Formation of the Face: The Mouth
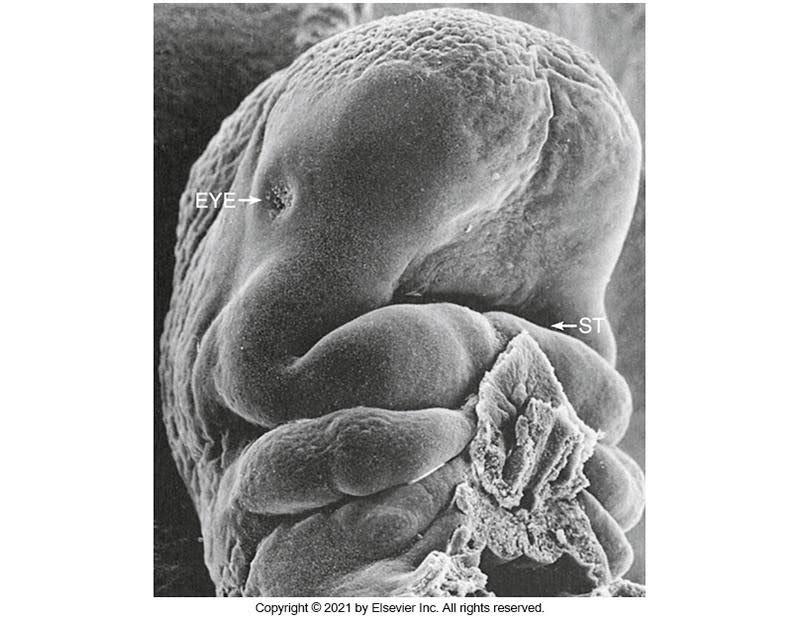
By the fourth week of development, the forming brain has grown rapidly over the oropharyngeal membrane toward the developing heart. At first, the oropharyngeal membrane separates the primitive pharynx (throat) from the amniotic cavity and fluid, but the membrane breaks down during the fourth week to form the stomodeum or primitive mouth.
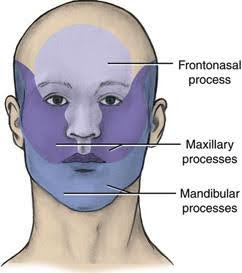
Beneath the stomodeum are six paired bulges of tissue called the branchial arches. These arches give the embryo the appearance of a fish with gills. The first branchial arches called the mandibular arches or processes, grow from either side toward the midline and fuse to form the mandible. At about the same time, additional swellings project from the mandibular arches in a superior direction to become the maxillary processes, which end up forming the midface.
The muscles of mastication are formed by the mesoderm, which makes up the mandibular arch and is innervated by the nerve of the mandibular arch, the trigeminal nerve. (Keep this fact in the back of your mind for now; it’ll make more sense in the next module, where we’ll learn about head and neck anatomy in more detail.)
Below is an electron microscope image of a human embryo in the fourth week of development, labeled with “EYE” and “ST” to indicate the early formation of the eye and somites.
Formation of the Face: Placodes
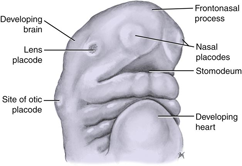
Let’s take a little closer look at the formation of the face starting in the fourth week of development, a critical time for the embryo, and continuing until the 12th week. A very prominent structure, the frontonasal process, forms at this time. This uppermost structure of the embryo will develop into the upper face and, as the name suggests, the nose.
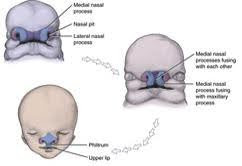
Placodes, the earliest signs of sense organs, arise during the frontonasal process of the embryo. There are lens placodes for the eyes and nasal placodes for the nose. The nasal placodes are of particular interest because they help form a portion of the midface. Initially, nasal pits (depressions) form at the site of the nasal placodes, and the area around these pits starts to grow into the medial and lateral nasal processes. The right and left medial nasal processes fuse to form the nose, philtrum, and tubercle of the upper lip. The upper lip is formed by the fusion of the medial nasal processes with the maxillary processes. In addition, the medial nasal processes begin to grow inward, yielding a structure, the intermaxillary segment, that will give rise to the primary palate. (More to follow on this).
 |
 |
|
Embryo at fourth week of development |
Development of the nose and upper lip |
Branchial Arches
By the end of the fourth week, six pairs of branchial arches have formed. The first branchial arch forms the lower lip, the muscles of mastication, and the anterior portion of the alveolar process of the mandible.
The second branchial arch, also called the hyoid arch, forms the styloid process, stapes of the ear, stylohyoid ligament, and part of the hyoid bone. This arch also forms the side and front of the neck and some muscles of facial expression.
The third branchial arch forms the posterior of the tongue and the body of the hyoid. The fourth, fifth, and sixth branchial arches form the structures of the lower throat and the muscles and nerves of the pharynx and larynx.
Test Your Knowledge
Formation of the Palate
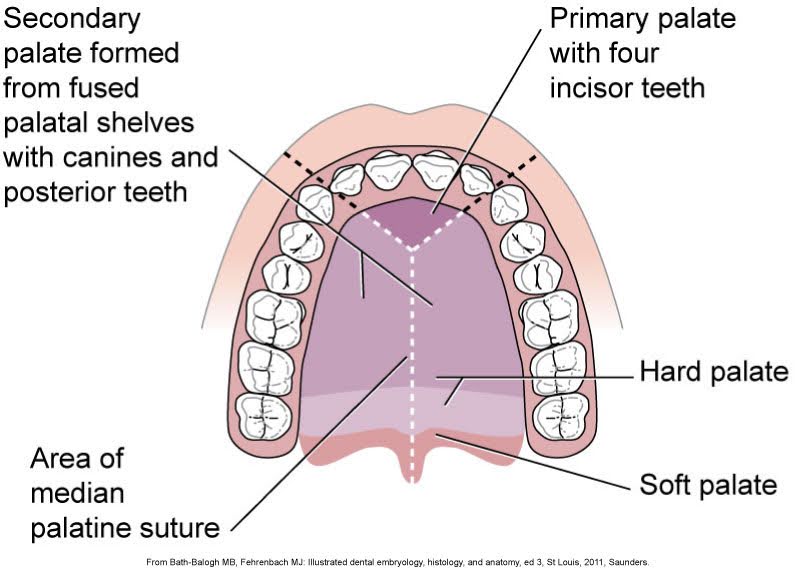
The hard palate is formed from a single wedge-shaped primary palate anteriorly and two secondary palates posteriorly. The primary palate forms first, during the fifth week, from the fusion (or joining) of the medial nasal processes that result in the intermaxillary segment. The term intermaxillary means “between the maxillary,” which describes the location of this wedge-shaped structure that will eventually become the anterior palate, the floor of the nasal cavity, and the nasal septum.
The secondary palate forms from the maxillary processes in the sixth week as vertical shelves that project inferiorly on either side of the forming tongue. Suddenly, the tongue drops down, and the palatal shelves close upward, like barn doors, toward the midline. In the final stage of palate formation, the palatal shelves of the secondary palate fuse in the midline and with the primary palate anteriorly.
In the diagram below, imagine that you are sitting on the developing tongue of the embryo, looking up at the palate as it forms.
Developmental Disturbances of the Palate and Lip
The diagram on the left below shows the contributions of embryonic structures to the face. The frontonasal process fuses with the maxillary processes to form the upper lip. Fortunately, the development of the face proceeds without a hitch in an overwhelming percentage of births, but on occasion, things do go wrong.
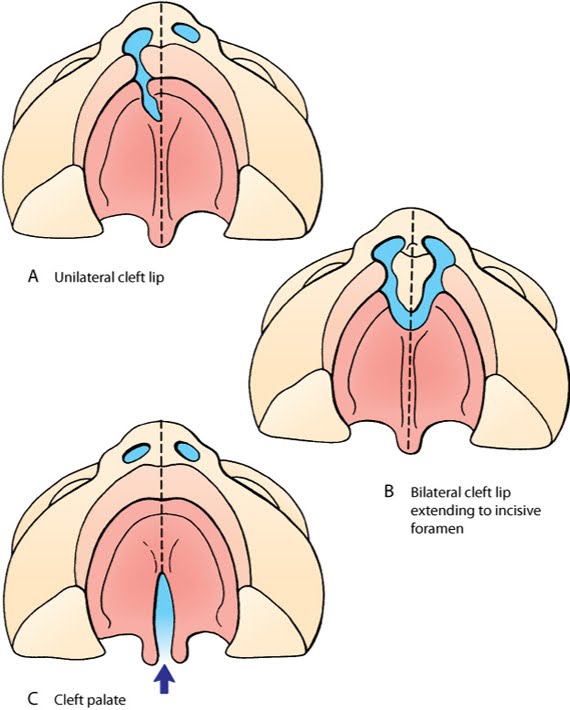
Clefts of various types occur when the fusion of the embryonic structures is incomplete. This can occur with the upper lip, either unilaterally (on one side; refer to image on the right below) or bilaterally (on both sides). A cleft may also extend onto the palate, where incomplete fusion may occur between the primary and secondary palate, between the right and left secondary palatal shelves, or both. Clefts occur in one in every 700 births. In many cases, clefts can be closed surgically, with excellent esthetic results.
 |
 |
|
Contributions of embryonic structures to the face |
An infant with a cleft lip |
The various types of cleft lip and palates are unilateral cleft lip, bilateral cleft lip extending to the incisive foramen, and cleft palate, which you will see illustrations of below.
Facial Development
The development of the human face occurs chiefly between the fifth and eighth weeks. The face develops from the frontonasal process and the first branchial arch. The face develops as follows:
- At one month, the overhanging forehead is the dominant feature.
- During the second month, the nose and upper jaw grow rapidly. The lower jaw seems to lag behind in growth.
- At four months, the face looks human, the hard and soft palates are beginning to form, and all primary dentition has begun to form.
- During the last trimester, fat is laid down in the cheeks in what is known as “sucking pads.” These give a healthy full-term fetus the characteristic round facial contours.
Video: Development of the Face and Palate [8:16]
Click here for a video transcript in .docx format: Video Transcript.
Test Your Knowledge
Facial Development After Birth
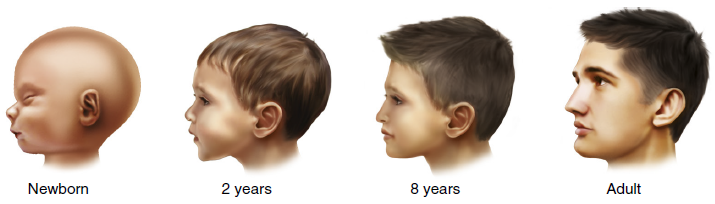
There is a considerable change in the shape of the face from that of a newborn to that of an adult. Most facial growth takes place during predictable growth spurts, which occur during youth and early adolescence. Facial bones grow and are reshaped to achieve normal growth and development of the face. This process involves the deposition (laying down) of new bone in some areas and the resorption (removal) of existing bone from others.
Take a moment to reflect: As you were growing up, did you notice that your face and jaws changed over time?
Tooth Movement
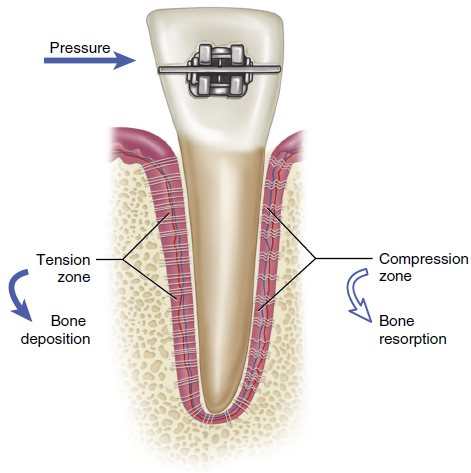
Remodeling occurs in response to forces placed on the tooth within its socket. Deposition is the process of “laying down,” or adding, new bone. Osteoblasts are the cells responsible for new bone formation. Resorption occurs when the body removes bone. Osteoclasts are the cells responsible for this process, in which bone cells are resorbed (taken away) by the body. Remodeling occurs in response to forces placed on the tooth within its socket.
Below is an illustration showing the process of orthodontic tooth movement with a tooth under pressure from braces, indicating the tension zone with bone deposition and the compression zone with bone resorption.
Test Your Knowledge
Tooth Development
The earliest signs of tooth development are found in the anterior mandibular region when the embryo is 5 to 6 weeks old. Shortly after the mandibular anterior teeth develop, the maxillary anterior teeth begin to develop, and the process of tooth development continues progressing towards the posterior in both arches. By the 17th week, all primary teeth are developed, and the development of permanent teeth has begun. At birth, there are normally 44 teeth in various stages of development.
Odontogenesis: Initiation, Bud, and Cap Stages
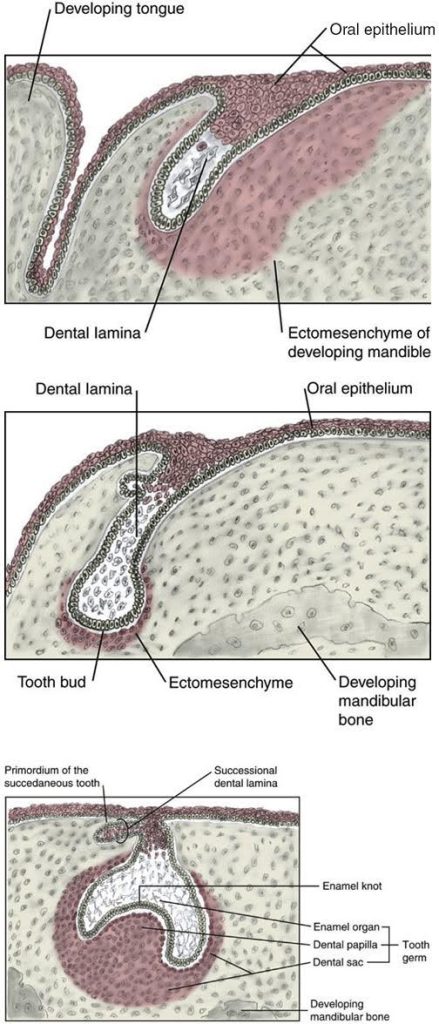
Odontogenesis, or tooth development, begins in the sixth week of development, during the embryonic period, with the thickening of the ectoderm lining the stomodeum to form the oral epithelium. The thickened oral epithelium consists of two horseshoe-shaped bands that will become the dental arches, maxillary and mandibular. The oral epithelium grows into the underlying tissue to form the dental lamina. This is called the initiation stage of tooth development.
The bud stage begins in the eighth week of development when the cells of the dental lamina proliferate (grow in number) to form 20 tooth buds, 10 for each arch.
The cap stage of tooth development begins in the ninth week with the growth of the bud into the enamel organ, which covers the forming dental papilla. The enamel organ, as its name suggests, will produce the tooth’s enamel, while the dental papilla will form the dentin and pulp. The developing tooth germ is surrounded by the dental sac, which will eventually form the cementum, periodontal ligament, and alveolar process.
Below are three sequential diagrams illustrating early tooth development stages: the top shows the dental lamina as it relates to the developing tongue and oral epithelium; the middle shows a tooth bud surrounded by ectomesenchyme in the developing mandible; and the bottom shows the tooth germ structure, including the enamel organ, dental papilla, and dental sac within the developing mandibular bone.
Odontogenesis: Bell, Appositional, and Maturation Stages
The next stage of tooth development is the bell stage, which begins in the eleventh week. The cells of the enamel organ and dental papilla begin to specialize for their particular role in laying down tooth structure. The enamel organ and dental papilla secrete the organic (non-mineral) components of the tooth. This material is called the matrix and is similar to steel rods embedded in a concrete structure. Enamel has very little organic matrix and is mostly composed of minerals (calcium). Dentin has more organic matrix material and is less mineralized and the pulp has more matrix and no minerals. Notice in the upper image to the right that the tooth bud for this succedaneous tooth has “sprouted” from the lamina of the forming primary tooth.
Next, the specialized cells of the tooth germ can begin laying down their matrix and building the substructure that will become the tooth. This is called the appositional stage. Enamel-producing cells are called ameloblasts and dentin-producing cells are called odontoblasts.
The final stage of tooth development sees the mineralization of the matrix in the maturation stage of tooth development.
Below are two diagrams of tooth development: the top illustrates the bell stage with labeled parts such as the enamel organ, dental papilla, and inner and outer enamel epithelium; the bottom shows a more advanced stage with labeled structures including ameloblasts, enamel matrix, dentin matrix, odontoblasts, and the pulp.
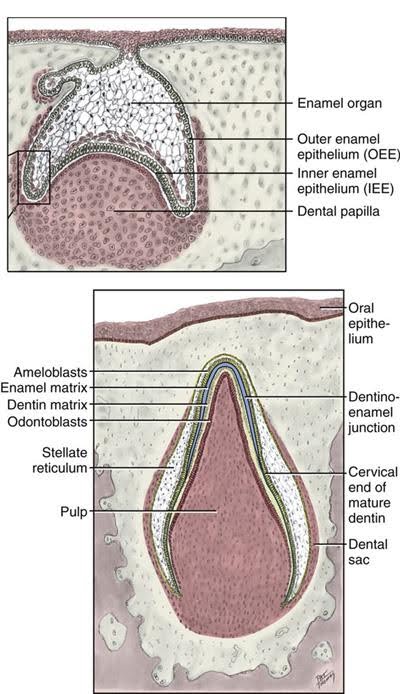
Let’s look a little closer at the appositional stage of tooth development. This critical stage begins with ameloblasts lining the hollow portion of the enamel organ opposite the odontoblasts of the dental papilla. Starting at the cusps or incisal edge of the tooth, these cells begin laying down a matrix to form the scaffolding for the tooth. The ameloblasts lay down the enamel matrix while receding toward the center of the enamel organ. At the same time, the odontoblasts lay down the dentin matrix while receding inward toward the center of the dental papilla. Unlike the ameloblasts, the odontoblast cells leave a projection within the dentin matrix called the odontoblastic process, while the cell bodies of odontoblasts line the pulp chamber. The dentinoenamel junction marks the starting point for matrix formation in the mature tooth.
At the cervical area of the tooth, the dental papilla continues to grow apically and lay down dentin, though no enamel organ is present to form enamel. Instead, cells from the dental sac transform into cementoblasts and line the newly formed root dentin. Cementoblasts produce cementum matrix to line the root dentin, thus forming the root of the tooth. The area where enamel ends and the cementum begins is called the cementoenamel junction.
Eruption and Exfoliation
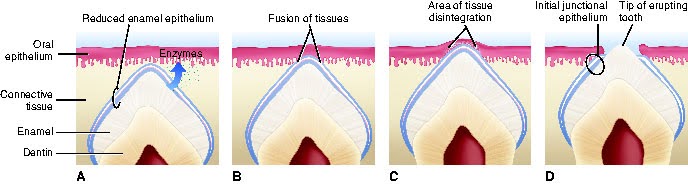
At a certain point in tooth development, it becomes time for the crown of the tooth to enter the oral cavity. As you know from personal experience, teeth erupt in sequence, generally starting with the front teeth and moving toward the molars. After enamel formation has ended for the developing tooth, the remainder of the enamel organ fuses with the oral epithelium of the oral cavity and creates a window through which the tooth crown will pass. Inflammation of the epithelium results in the pain and swelling commonly associated with teething. From that point on, teeth erupt into the oral cavity through some unknown force.
Odontoclasts and osteoclasts are cells that eat away at tooth structure and bone, respectively. These cells are responsible for resorbing the roots of primary teeth in preparation for exfoliation or shedding to make room for their permanent successor. As more and more root and surrounding bone is resorbed by the “clast” cells, the primary tooth’s crown becomes looser and looser until it falls out (or is extracted by a dentist or parent). The permanent tooth follows the path created through the epithelium and into the oral cavity.
Below are sequential diagrams illustrating the process of tooth eruption: A) Enzymatic breakdown of reduced enamel epithelium, B) Fusion of tissues, C) Tissue disintegration creating a path for the tooth, and D) Tooth emerging through the oral epithelium.
Developmental Disturbances
Disturbances at any stage of dental development may cause a wide variety of anomalies (abnormalities). These can be caused by genetic and environmental factors.
In prenatal tooth development, genetic factors such as tooth and jaw size are most often of concern. A child may inherit large teeth from one parent and a small jaw from the other parent.
Environmental factors are adverse environmental influences called teratogens, including infections, drugs, and exposure to radiation. Any drugs, whether prescribed, over-the-counter, legal, or illegal, including alcohol, may cause an anomaly if taken during pregnancy. A mother’s oral health is also a concern. Toxins from an oral infection may be dangerous for the mother and baby.
Test Your Knowledge
Dental Anomalies: Alteration in Tooth Number
Many conditions of teeth can be traced directly to a problem occurring during tooth development. Here are some examples of dental conditions related to the initiation stage of tooth development:
- What would happen if, instead of 32 permanent tooth buds forming, only 31 formed? If you guessed that a missing tooth would result, you are right! The term given to congenitally missing teeth is anodontia. The condition may involve a single tooth or many teeth, though the latter is usually the result of a syndrome such as ectodermal dysplasia (mentioned earlier). Commonly missing teeth include the third molars and maxillary lateral incisors.
- The opposite situation can occur as well. If 33 permanent tooth buds form instead of 32, the extra tooth is known as a supernumerary tooth. Fourth molars aren’t uncommon; they’re called distomolars or distodens. A third maxillary central incisor can erupt in the midline; this is called a mesiodens.

Dental Anomalies: Alteration in Tooth Shape and Size
Teeth can grow with an uncharacteristic shape or size due to a disturbance in the bud or cap stage of tooth development. Here are some examples:
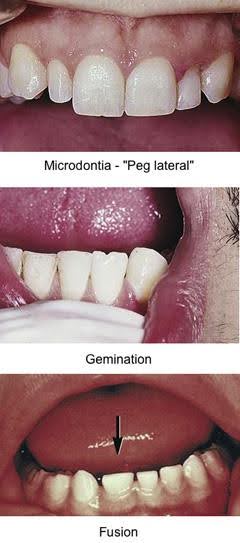
- Teeth that are smaller than usual exhibit a condition called microdontia. Maxillary lateral incisors with this condition are called “peg laterals.” Third molars are also commonly affected.
- In macrodontia, teeth are larger than normal.
- Gemination is a condition in which the tooth germ divides, leaving a large, divided crown sharing a single root. In gemination, the number of teeth in the dentition is normal.
- Fusion is similar in appearance to a tooth that has undergone gemination, except that fused teeth result from the joining of adjacent tooth germs to form a single large tooth. Fused teeth generally have separate roots, and the dentition has one less tooth than normal.
Dental Anomalies: Problems with Apposition and Maturation
Teeth that are very weak or display severe discoloration may result from poorly laid enamel or dentin matrix in the appositional stage or faulty mineralization in the maturation stage. These conditions can be localized to a few teeth or be generalized to the whole dentition. Here are some examples:
- An example of a localized enamel hypoplasia is Turner’s spot, which is a discoloration of the permanent crown resulting from traumatic injury to the primary tooth that forces the primary root into the developing tooth germ.
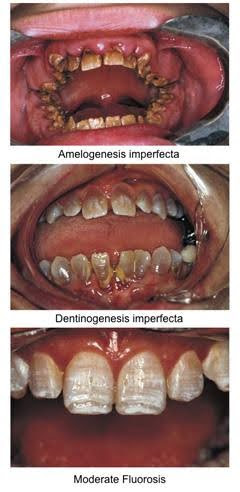
- Amelogenesis imperfecta is a hereditary condition that results in generalized weak enamel that fractures off, leaving the underlying dentin exposed and vulnerable to wear.
- Dentinogenesis imperfecta is a hereditary condition that results in weak, discolored (brown to blue-gray) dentin. This weak base for the normal enamel that overlies the dentin causes the enamel to fracture.
- Too much fluoride can cause enamel dysplasia, which is called fluorosis. The teeth exhibit staining and are mottled in appearance.
Activity 3: Dental Anomalies
You have completed Module 1. Please return to Blackboard for the next steps.
Media Attributions
- Images from: Modern Dental Assisting, 13th and 14th Edition
(em-bree-OL-uh-jee); The study of prenatal development, from conception to birth.
Development stage of human development that starts at pregnancy and ends at birth.
Union of the male sperm and the female ovum.
(jes-TAY-shun); Stage of human development that starts at fertilization and ends at birth.
The stage of development that occurs during the first week after fertilization.
Fertilized egg.
(em-bree-ON-ik); Stage of human development that occurs from the beginning of the second week to the end of the eighth week.
An organism in the earliest stages of development.
Stage of human development that starts at the beginning of the ninth week and ends at birth.
An embryonic human from two months after conception to birth.
(mye-OE-sis); Reproductive cell production that ensures the correct number of chromosomes.
The outer layer of the three primary embryonic layers.
The middle layer of the three primary embryonic layers.
The inner layer of the three primary embryonic layers.
The primitive mouth.
The earliest signs of sense organs, arise on the frontonasal process of the embryo.
Rectangular area from under the nose to the midline of the upper lip.
The shelf that separates the oral and nasal cavities.
The second branchial arch, which forms the styloid process, stapes of the ear, stylohyoid ligament, and parts of the hyoid bone.
The final palate formed during embryonic development.
The process by which the body adds new bone.
(OS-tee-oe-blasts); Cells that for bone.
(OS-tee-oe-klasts); Cells that resorb bone.
(o-don-to-JEN-eh-sis); Formation of new teeth.
Thickened band of oral epithelium that follows the curve of each developing arch.
Enlargements produced by the formation of dental lamina.
Part of a developing tooth destined to produce enamel.
Gingivae between the teeth.
Connective tissue that envelops the developing tooth.
(suk-se-DAY-ne-us); Teeth permanent teeth that replace primary teeth.
(uh-MEL-oe-blasts); Cells that form enamel.
(o-DON-to-blasts); Cells that form dentin.
A projection left by the odontoblast cells within the dental matrix.
(se-MEN-toe-blasts); Cells that form ameloblast.
Area where enamel ends and the cementum begins.
Cells that are responsible for resorbing the roots of primary teeth in preparation for exfoliation.
(eks-foe-lee-AY-shun); The normal process of shedding the primary teeth.
Absence of single or multiple teeth.
Development of one or more extra teeth.
A third maxillary central incisor can erupt in the midline.
