6 Chapter 6: Glitches in the Brain and Consciousness
The Essential Neuroscience of Human Consciousness
The Essential Neuroscience of Human Consciousness
Amedeo D’Angiulli
Chapter 6: Glitches in the Brain and Consciousness
6.1. Epileptic seizures and Consciousness
6.2. Medial-Temporal Lobe Amnesia & Consciousness
6.3. Syndromes of Transient Amnesia and Consciousness
6.4. Left and Right Hemispheres
6.5. Out-of-Body and Near-Death Experiences
6.6 Neuropsychological Visual Syndromes and Phenomenal Consciousness
6.7 Drugs and altered states of consciousness
6.7.1 Ego dissolution
6.7.2 Lysergic acid diethylamide (LSD) and ego dissolution
Chapter 6. Glitches in the Brain and Consciousness
6.1. Epileptic seizures and Consciousness
Epileptic seizures are temporary glitches of varying severity in the brain that can temporarily affect consciousness. Therefore, the study of these glitches becomes interesting and very relevant to understand how consciousness is implemented in the brain. There are three main types of epileptic seizures: Absence seizures (petit mal), generalized tonic-clonic seizures (grand mal), and complex partial seizures.
Absence seizures last less than 10 seconds and manifest as brief lapses in awareness, with a characteristic fixed stare. These seizures seem generated by thalamocortical oscillations. During one of these seizures, EEG shows characteristic 3-4 Hz (lower theta) spike-wave discharges. The temporary impairment of consciousness associated with the seizures is very variable. Severity varies with the task; it is minimally affected in repetitive motor tasks but much more difficult to recover consciousness & cognitive engagement in decision/verbal tasks.
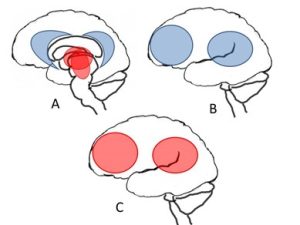
The fMRI changes during spike-wave discharge in absence seizures have a very specific bilateral increased activation in the upper brainstem and medial thalamus, bilateral decreased activation in the midline anterior and posterior inter-hemispheric regions (anterior and posterior cingulate, medial frontal cortex, precuneus) and activation decreases & increases in the lateral frontal and parietal cortex. Therefore, brain activation during seizure (ictal) can be described by Figure 7’s sequence A, B, C. After seizure (postictal), the activation pattern can be again described by a very similar sequence A (interhemispheric only), B, C.
Generalized tonic-clonic seizures are characterized by bilateral tonic limb rigidity (10-20 sec) followed by rhythmic bilateral clonic jerks (1 min). They typically last 1-2 minutes in total. After the seizure, the individual may feel sleepy, confused and weak. EEG activity shows a very distinctive pattern. In the tonic phase, generalized high-frequency polyspikes occur. In the clonic phase, generalized polyspikes are followed by or overlap with a massive wave. In the postictal phase, it is possible to observe generalized lower amplitude waves and a generalized slowing of the EEG. Calling tonic-clonic seizures “generalized” is not very accurate because it may not be generalized, but rather depend on focal abnormal activity. Two types have been identified: one primarily generalized (with no obvious focal onset) and another secondarily generalized (focal onset followed by wide-spreading).
A major source of information regarding tonic-clonic seizures is derived by ictal-interictal SPECT (Single-Photon Emission Computerized Tomography) studies. In the SPECT technique, researchers inject the radioisotope tracer before or when the seizure is starting, but imaging is done when the patient is stable and immobile. Therefore, imaging reflects the CBF changes during the seizure. The ictal-interictal period has been studied in both spontaneous and induced (via electroconvulsive therapy) tonic-clonic seizures. Activation patterns with SPECT have shown that during seizures, there are increases in CBF of the thalamus and upper brainstem, decreases in the anterior and posterior cingulate gyrus and increases in the lateral frontal and parietal cortex. In contrast, during the postictal period when there is unconsciousness, there are CBF decreases in the anterior and posterior cingulate gyrus, decreases in the lateral frontal and parietal cortex and increases in cerebellum. Notice that all the effects are bilateral. Thus, the ictal pattern shown in Figure 7 would correspond to the sequence of fMRI activation A, C, while the postictal pattern would correspond to A (interhemispheric), B.
It is important to notice that what triggers the loss of consciousness seems to be independent from what triggers the motor behavior and convulsions. When the focus and spread of seizures that lead to loss of consciousness occurs in the connections between frontal and parietal cortices, the motor areas are spared from this increase in activity. Thus, tonic-clonic movements are mediated through an indirect pathway starting from the brainstem to the motor cortex, rather than the direct pathway to the motor cortex via the cerebellum. When the focus and spread of seizures occurs in the motor cortex, the conscious systems of frontal and parietal areas are unaffected and there may not be loss of consciousness.
In contrast to the two previous types of seizures, complex partial seizures involve unilateral focal regions (most often the temporal lobe). Partial simple seizures do not involve loss of consciousness, whereas complex partial seizures do involve it. The progression of complex partial seizures generally begins with an aura (a premonition, fear, anxiety or panic-like feeling), followed by a fixed stare, unresponsiveness, automatisms, chewing, lip-smacking and unconsciousness. The duration of such a progression is typically 1-2 minutes. EEG shows a prevalence of 5-7 Hz waves in the temporal lobe, as well as slow waves. The impairment of consciousness is relatively long as it is also followed by a state of confusion which lasts long into the post-ictal period. A classic sign of this type of seizure is amnesia, typically linked with temporal lobe dysfunctions. Therefore, when looking at Figure 7, the brain activation in complex partial seizures shows an ictal pattern of A, B, whereas it shows a postictal pattern A (interhemispheric), B.
The most influential theory that explains why there is loss of consciousness during complex partial seizures, supported by EEG and CBF neuroimaging studies, is the Network inhibition hypothesis. The idea behind it is that a focal seizure in the temporal area propagates to disrupt adjacent upper brain and thalamic input to fronto-parietal associative cortices and their connections. What happens in other types of seizures is similar. To summarize the findings, all three types of seizures involve an increase of thalamus, upper brainstem, lateral frontal and lateral parietal activity. The difference is in the temporal sequence and direction of activation; there is a mixture of increase and decrease in absence, increase in tonic-clonic, and decrease in complex partial seizures. However, when consciousness is lost (as in most cases) during the postictal period, such loss of consciousness always correlates with decreased activity in fronto-parietal areas and their connections.
6.2. Medial-Temporal Lobe Amnesia & Consciousness
The syndrome of medial-temporal lobe (MTL) amnesia is a condition that is invariably and inevitably linked with what is perhaps the most famous case study in the history of neuroscience: H.M., or Henry Molaison. H.M. suffered a pervasive and debilitating form of status epilepticus with very frequent tonic-clonic seizures with a period of one hour. In the 50s, while he was in his mid-twenties, he underwent a completely explorative and unprecedented neurosurgical procedure which left him without his hippocampus and part of the medial temporal lobe. The most evident feature of his amnesia is illustrated by the contrast between anterograde (before insult) and retrograde (after insult) memory as reflected by memory of famous faces. In MTL amnesiacs, the rate of correct anterograde memory for famous faces is generally good (50-75%). However, retrograde memory drops to 0-20% recognition. In normal individuals, the memory function is reversed; remote memory for famous faces is very poor (~30%) but very good for recent items (75%).
However, things are much more complex. Memory of periods before (but not just before) insult is actually superior in MTL patients than normal controls; perhaps because it has less interference from incoming info in nearby periods. Thus, anterograde amnesia involves specific deficits: the inability to learn new information despite the ability of retrieving memories before the insult, and the inability to hold information in short term memory (STM) or transferring it from STM to long term memory (LTM). Many other cognitive abilities are spared, as reflected by neuropsychological testing correlates of MTL. Depending on the nature and extent of their lesions, MTL patients usually achieve a normal performance (memory excepted) on neuropsychological test batteries that probe residual cognitive functions, such as the Mini Mental State Exam, Boston Naming Test, Wisconsin Card-Sorting Test and the full IQ scale of the Wechsler Adult Intelligence Scale-Revised (WAIS-R). Memory impairment becomes obvious on delayed list recall as measured by tests such as the California Verbal Learning Test (CVLT), Wechsler memory Scale (WMS) and Rey-Osterrieth complex figure recall.
The neuroanatomical and neurophysiological correlates of MTL typically show circumscribed lesions involving damage to the MTL-diencephalic system, including the hippocampal complex and adjacent structures. The relevant aspect for the study of consciousness is that even H.M., who showed extensive neural damage, had many parts of the cortex intact and especially parietal and frontal areas. Most of the thalamus was intact, as well as areas corresponding to the default networks. In other words, most of the system of consciousness was spared. Thus, in this context, the question that is important to explore is what, if any, relationship exists between the neural substrate of amnesia and the contents of consciousness.
Neuroimaging data collected with SPECT showed that during most tasks, H.M. had no brain activity in MTL but normal activity in other parts of the brain. fMRI showed some MTL activation related to a novel picture encoding task. However, surgically produced neurotoxic lesions that targeted the MTL (but spared the hippocampus) in rats and baboons have shown impaired recognition memory and hypometabolism not just in the MTL but in many other areas, including frontal and parietal cortices. Therefore, it is not clear if lesions sufficient for anterograde amnesia also affect consciousness and phenomenology. Of course, animal models cannot answer this key question.
Consciousness of memories is quite different from consciousness of perception. The format in which memories are stored is different from the pattern of neuronal firing that supports consciousness during perception or thought. To retrieve our memories, we need to convert them from implicit, dormant neuronal activity patterns to explicit neuronal activity. During memory retrieval, conscious recall corresponds to the reenactment of a precise pattern of neuronal firing used to encode an episode in our life. Conscious awareness of recall is therefore related to declarative or explicit memory. When you are conscious of something or of your awareness, you are using a part of declarative memory called autonoetic memory. It is associated with the conscious experience of memory as refers to the self and autobiography (extended consciousness). This latter sub-part of declarative memory is known as episodic memory. In contrast, noetic memory is for pieces of general impersonal knowledge, such as geographical knowledge surrounding Canada’s capital. This other part of declarative memory is also called semantic memory. Finally, the other recall system is anoetic memory, which is the memory of performance, abilities and skills influenced by past experience but without awareness of it. Anoetic memory is part of implicit (non-declarative) memory.
Two major memory models associated with declarative and implicit memory systems have been postulated as the processes underlying memory: 1) Learning/encoding (via consolidation) and 2) Retrieval (via organization of storage). Although these mechanisms are not mutually exclusive, pieces of their models have been compared to try and explain amnesia. In particular, one influential line of experimental research showed that item recall, after exposure to a list (usually words or pictures) that needs to be remembered, can be facilitated if there are cues associated to the items (cued recall). For example, giving labels or categories for the list such as “animals”, “foods”, “tools”… The second re-test exposure usually did not produce good rates of implicit recognition (i.e., discrimination between old/already seen vs. new/unseen items), unless recognition was again cued.
Interestingly, when experimenters tried to help memory recall in amnesiacs, implicit memory repetition priming (not conscious cued recall!) worked in these patients. This suggests that some memory deficits observed in MTL amnesia are due to impairment of declarative memory and “binding”. The latter is the consolidation process by which a transfer of information from perception to memory occurs, which allows retrieval via conscious awareness and volition. Further evidence for the idea that amnesia is an impairment of consolidation is that although damage to MTL produces anterograde amnesia, there is also some retrograde amnesia. However, retrograde amnesia related to this damage is unstable and depends on many factors at insult. Importantly, MTL retrograde amnesia is “graded”, with more memory loss just before insult and less for years before insult. To explain all the data research has given us, the standard consolidation theory proposes that there may be a time-limited role of MTL in the formation of memories. Memory for information learned (encoded) shortly before insult is vulnerable to disruption because consolidation is still underway. The MTL continues to play a role in memory processing for some time after initial encoding.
More recently, another hypothesis called the Multiple trace theory (MTT) has been put forward, which postulates that every new memory generates a new trace. For example, an Episode X generates multiple traces of X. With repetition, common elements of the X traces create a representation of X (semantic knowledge) independent of the particular episodes or experiences linked with X. It is independent from the concrete, perceptual and sensory aspects of X, but preserves its essential meanings. According to MTT, such “trace construction” depends on the hippocampus. Both standard consolidation theory and MTT predict that if the MTL is damaged, then the semantic independent knowledge is not destroyed. According to MTT, however, the autobiographical experience of X will be extremely deteriorated (especially with hippocampal impairment). Standard consolidation predicts no difference with normal memory of the same vintage (i.e., of the same time/age period). Nevertheless, a difference remains in phenomenology and consciousness of memory recall, which involves recollection as opposed to familiarity. Recollection is detailed recall of identity and context of the remembered object (knowing who, what, where, when). Familiarity is a general feeling of already knowing something.
This battle of theories has not yet yielded a winner. Rather, some researchers think that the theories don’t truly differ and that their differences can be reformulated with questions. For example, are there two different mechanisms for qualia, one for recollection and another for familiarity? Or is there one process with different strengths that explains both types of qualia, i.e.: “stronger familiarity” leads to recollection? Similarly, there might be a dual process or anatomical mechanism whereby the hippocampus supports recollection and other MTL areas support familiarity. Others posit it could be a single process, a distributed contribution of the MTL to memory. Different distributions of neural connections and their strengths might lead to both forms of qualia.
Whatever the underlying cognitive mechanism, much evidence points to the role of the hippocampus in STM. First, the hippocampus influences learning or representation of the relationships between items in the environment (relational binding). Relational binding may be related to representing the links between two objects, which are various types of information. This ability seems disrupted in patients with hippocampal damage and is shown in STM tests with delays as small as 1 second. Second, the hippocampus seems involved in imagination of future scenarios (prospective memory). Bilateral hippocampal damage is correlated with less vivid imagery and less spatial coherence in mental images (less contiguousness and spatial integrity).
Finally, one may wonder “What it is like to be an amnesiac”? In the phenomenological stream of consciousness in amnesiacs, subjective time seems experienced much faster for periods that last more than 20 seconds. A paradigmatic example is from the verbalizations collected in many videos available from the internet and other sources by another famous amnesiac, Clive Wearing, a former music conductor and expert who suffered major impairment of the MTL. From his verbalizations, it is clear that he seemed to experience life with amnesia in a state philosophically known as fringe consciousness. It has been estimated that Wearing’s and H.M.’s reports and behaviours fitted a distorted sense of time: 1 hour corresponded to 3 minutes, 1 day corresponded to 15 minutes and 1 year corresponded to 3 hours. That is, he lived without stability, continuity and reassuring permanence that the background of awareness provides to most individuals.
6.3. Syndromes of Transient Amnesia and Consciousness
The syndromes of transient amnesia are another umbrella category, including glitches in the brain that affect the consciousness of memory. Three main clinical syndromes will be discussed: transient global amnesia, transient epileptic amnesia and psychogenic amnesia.
Transient global amnesia (TGA) in an abrupt onset of profound but transient anterograde amnesia, with a variable degree of retrograde amnesia. Its clinical features include that the onset is an event witnessed by observers, amnesia is the only impairment, there are no neurological signs during and after the episode, there is no epilepsy or head injury and it is resolved within 24 hours of onset. This syndrome is infrequent (3-10 cases per 100 000 people) and its recurrence very rare. The mean age of people experiencing it is 62 years, and it occurs only between 40 and 80 years of age with no gender differences.
Retrograde amnesia, whether minimal or extensive, recovers much more quickly than anterograde memory. Notably, there are no impairments of consciousness and no impairment of knowledge of personal identity; the only potentially permanent impairment is the gap of the attack itself. The immediate period before and after the amnesic episode may be completely erased from memory.
TGA is usually preceded by intense emotional and/or physical stress. It is not caused by epilepsy; EEG is normal and TGA attacks are not recurrent. Migraines and possibly a spreading metabolic depression in the hippocampus have been proposed as causes, but the age of occurrence and frequency do not fit migraine patterns (patients are older than expected). A more plausible hypothesis is that individuals who experience TGA may have micro-strokes. They would have temporary venous ischemia in the medial temporal and diencephalic regions with transient ischemic strokes in the hippocampus. On the other hand, data shows that acute psychological stress (ex: anxiety and panic attacks) can cause hyperventilation, which can then reduce CBF in medial temporal regions and cause amnesia.
Neuroimaging evidence seems consistent with the last explanation. 24-72h from onset, MRI scans reveal small, 1-2 mm punctuate lesions in hippocampal regions vulnerable to hypoxic injuries. After a few months, these lesions heal and memory is back to normal. Neuropsychological testing shows that patients in TGA attacks have no major impairment of working memory but have a pattern similar to medial-temporal amnesia. Performance on delayed long-term anterograde memory is minimal and priming tasks show intact implicit memory. In the acute and recovery phases, retrograde memory seems impaired in autobiographical features. Anterograde impairment lasts much longer than retrograde, going on for days or even months. Amnesia for events during, and 1-2 hours prior to, the attack is permanent and complete.
Transient epileptic amnesia involves a history of recurrently witnessed episodes of transient amnesia where cognitive functions are otherwise intact. It is associated with one or more symptoms of epilepsy such as an abnormal epileptiform EEG, clinical signs of complex partial seizures and a good response to anticonvulsant therapy. Several clinical features can help identify this type of syndrome. Typically, it begins in late middle to old age (mean 62 years). It manifests as mixed patterns of anterograde and retrograde amnesia with considerable variation in their extent. However, the individuals who experience these episodes have normal cognitive functions; most of them do complex actions, which they complete, when an episode occurs. During these amnesias hallucinations of smell or taste are typical. Episodes may last from 30 minutes to an hour and may reoccur at a rate of around 13 episodes a year.
Amnesia is often linked with awaking from sleep. The temporal lobe and hippocampus seem involved, as in MTL amnesia and temporal-lobe epilepsy. There are three types of persisting memory deficits:
- Accelerated long-term forgetting: Quicker forgetting for retention of information in LTM within 3 weeks to 2 months
- Considerable loss of autobiographical memory associated with focal retrograde amnesia: Significant impairment of remote memory with intact anterograde memory
- Impairment of topographical memory for familiar routes.
Psychogenic amnesia is defined as atypical forgetting not due to injury, insult or disease of brain tissue, being instead attributable to a certain psychological event. It can be situation-specific, responding to an emotionally “charged” event, or global. This type of amnesia typically follows a stressful financial or marital crisis, with depression and alcohol abuse in the background. Anterograde memory is preserved but impairment affects personal identity and autobiographical knowledge. Recovery is often protracted and incomplete.
Other types of transient amnesias can be caused by head injury. Head injury of any intensity can produce fully reversible retrograde amnesia, except for the instants preceding the injury. TGA can be triggered in younger people that sustain head trauma and may be recurrent. Additionally, several drugs, anesthetics or even alcohol can produce short anterograde amnesia by impairing encoding. Drugs like benzodiazepines act on GABAa receptors in the hippocampal complex, strongly affecting declarative memory.
Transient amnesias offer a very coherent picture of temporary glitches of consciousness. Wakefulness and functions that depend on it are unaffected, while awareness of the self and its surroundings is there but altered. Patients recognize with perplexity that they are unable to remember information from a few minutes before. The most important effect of transient amnesia is on consciousness of the self and the loss of autobiographical context. In other words, there is impairment of extended consciousness while core consciousness remains mostly intact.
6.4. Left and Right Hemispheres
A certain neurosurgical procedure, the callosotomy (split-brain), involves cutting all or part of the corpus callosum, disabling communication between the two hemispheres. This procedure is still used in rare cases to treat epilepsy or tumors. Patients in this condition revealed unique specializations in their hemispheres but also glitches in what was conscious or not in them. Interestingly, no changes in personality or mental illness were observed. No problem of the dominant-hand right side was observed but impairment was observed on the left side; there was inability to identify an object (agnosia), name it (anomia) or draw it (agraphia). Visually speaking, there were problems in the left visual field. Language (written and spoken) is specialized in the left hemisphere, with some very limited spoken abilities in the right hemisphere. However, writing in the right hemisphere can be intact and better than in the left. Different types of knowledge are stored and used in each hemisphere. Specifically, the left one seems specialized in problem-solving and rich lexical semantic knowledge, such as drawing inferences (verbal, linguistic and spatial). The right hemisphere seems specialized in spatial analysis and perception. In spite of these clearly different functional specializations, the two hemispheres have a lot of overlap and redundancies. This is especially notable for memory processes which seem less lateralized and more distributed.
Anosognosia is a condition in which split-brain and other patients with impairments of consciousness deny anything is wrong with them, in spite of clearly observable effects of brain injury. The best example of this is perhaps another neuropsychological syndrome, hemispatial neglect. Neglect is usually caused by a stroke in the right parietal cortex; it disrupts attention and awareness to the left side of space. Accordingly, a patient only performs actions in half of their visual field, seeing, dressing or eating only on the left side. However, these patients do not sense there is something wrong with them and deny any problems.
A possible explanation for this glitch of consciousness has been proposed by Michael Gazzaniga. His main idea is that consciousness and awareness for an element is completely dependent on a specific module. Therefore, hundreds of functions are controlled by hundreds of modules. If the module controlling function X is impaired or has no input, it can then alert the whole system that something is wrong. However, if the module itself is removed, the communication of its status does not occur. Consequently, nothing is noticed or acknowledged (out of sight, out of mind). But then, how does consciousness keep it together? How is unity of consciousness achieved? Gazzaniga has proposed that specialized and localized neural networks send information about their status to another specialized system, the interpreter. The interpreter is uniquely human and located in the left hemisphere. If the interpreter does not get information about a module, it compensates by changing the conscious experience of both hemispheres and concocting rational or fictional explanations. According to Gazzaniga, this is the best explanation of why research in split-brain patients ultimately reveals that the left hemisphere does not “miss” the right hemisphere at all! That is, it seems like the left hemisphere is sufficient for all consciousness. Of course, it also fits the idea that this is yet another form of anosoagnosia (unconsciousness or denial of an impairment) which may actually be a major impairment to the right hemisphere. At this point, Cazzaniga’s consclusion is an interesting one but is just a speculation.
6.5. Out-of-Body and Near-Death Experiences
An interesting and weird phenomenon involving glitches in consciousness concerns the out-of-body experience (OBE). OBE involves the occurrence of three key qualia:
- Disembodiment: A feeling of being outside one’s physical body
- Perspective: Perceiving the self as localized at a distant, elevated visuo-spatial point
- Autoscopy: The experience of seeing one’s own body from that elevated perspective.
The incidence of this strange phenomenon is difficult to establish accurately, as research efforts have so far involved different questions and methods, while most studies have sampled North American and European undergraduate students in psychology. As a result, the estimated incidence projected on the general population shows extreme variations in these studies, ranging from 8% to 34%. A more conservative (and plausible) estimate of incidence in the general population is ~5%. Indeed, it is very difficult to see and measure this phenomenon, since only one or two authentic OBE episodes are experienced by individuals in their lifetime.
Precipitating factors likely associated with OBEs are neurological conditions, such as epilepsy and migraines, as well as vestibular dysfunctions (especially impairments affecting the otoliths). OBE typically occurs when the body is supine, and a group of individuals who seem more susceptible to it are professional pilots. The neuroanatomical substrate of this glitch seems to be the temporal-parietal junction (TPJ). Other states of consciousness seem to be related to OBE, such as schizophrenia and altered states deriving from substance use (LSD, marijuana). Additionally, insufficient anesthesia and muscle relaxants seem promote feelings of awareness with paralysis; visual awareness at that time may be associated with OBEs.
A pattern of brain activity observed during cardiac or post trauma surgery seems to reveal a possible model of what happens in the brain. An initially increased awareness is associated with CBF decrease at the beginning of anesthesia, with hemodynamic changes in TPJ. These observations have led to the plausible hypothesis that OBE may result from failure to integrate multisensory bodily information involving disintegration of personal and extrapersonal space (coordinated by neural networks in the TPJ).
Near-death experiences (NDEs) typically consist of phenomenological experiences of vivid hallucinations and strong mystical or emotional feelings during perceived life-threatening situations. All situations we have encountered so far that lead to traumatic brain injury have been associated with NDEs. Most of our knowledge about NDE, however, comes from cardiac arrest patients. NDE incidence in these self-selected populations is much higher than one might expect, hovering around 42-48%. Estimates of occurrence in the general population are much lower and range between 6-12%. Sex and age at trauma seem to be good predictors, as women report more NDEs and the younger, the more likely
Much effort has gone into defining the qualia involved in NDE. For example, Greyson’s NDE scale reduces the syndrome to three types of experiences: Cognitive, Affective and Transcendental (paranormal). One or more of OBE’s three aspects (disembodiment, autoscopy, perspective) is a key feature in NDE. Very often, they involve the actual or imagined scene of the accident and operating room. A few reliable findings suggest that autoscopy and “seeing lights” are reported more vividly and frequently in people who are actually close to dying as opposed to people who believe they are dying. Overall, however, the most consistent experiences are imagery of the tunnel and light, the life review, meeting spirits and extremely positive and negative emotions. Other minor features involve hyper-realness (that is, more “vivid” than real perception itself) and mental clarity (extreme vividness), a distorted sense of time, mystical experiences and a border on (and return from) death. However, some psychological aspects of personality seem to be good predictors of NDEs in addition to trauma, such as absorption. This is the tendency to have vivid hallucinations, imagination, daydreaming and enhanced sensory experiences.
NDEs may fit not one but multiple neurological syndromes associated with cortical damage in the frontal and occipital cortices, basal ganglia, hippocampus and thalamus, but the brainstem is spared. Brain anoxia (complete lack of oxygen) or brain hypoxia (reduction of oxygen) in cardiac arrest can have similar effects to general anesthesia. Additionally, complex partial seizures, as well as temporal lobe & hippocampus spike activity, have been reported post-NDE in non-epileptic patients. This overlaps with some resulting aspects of temporal lobe amnesia (graded retrograde and severe anterograde loss of memory around the moment in which the impairment/accident occurred). Direct cortical electrical stimulation has shown that memory flashbacks that occur during NDEs can be elicited by stimulating the TPJ and hippocampus. Overall, research suggests that NDEs have two main types.
- Type 1: Predominantly right hemispheric with major right TPJ impairment. OBE and lack of gravity, distorted time, silence (peace)
- Type 2: Predominantly left hemispheric with major left TPJ impairment: Mostly sensory experiences and presence of, or meeting with, other entities.
Of course, it is entirely possible to have a combined form of NDE resulting from bilateral TPJ impairment.
6.6 Neuropsychological Visual Syndromes and Phenomenal Consciousness
Visual phenomenal consciousness is defined in operational terms as conscious reportability, the ability to explicitly report to oneself or someone else the object of our visual perception. But, we know from behaviourism (recall John B. Watson and R. Skinner) that subjective and conscious verbal reports, historically called introspection, can be biased and tell us less than what the brain processes. They’re also known to be unreliable, so why bother?
It turns out that behaviourists may be right in saying that introspection can be a wrong method to inquire about the mind and consciousness. Scientists obviously cannot rely on naïve human observers to understand how everything works. Similarly, those accounts cannot be taken literally, as when people claim to have seen spirits, dead relatives and started to fly. Even so, for all these reports – if they are not lies – there must be a neuroscientific explanation. As we have discussed in Chapter 1, simply eliminating them does not serve us well in pursuing the study and understanding of human consciousness. Thus, introspection and self-reports can be used as raw data. This is beautifully illustrated by a quote from Stanislas Dehaene (2014; p.12):
“The correct perspective is to think of subjective reports as raw data. A person who claims to have had an out-of-body experience genuinely feels dragged to the ceiling, and we will have no science of consciousness unless we seriously address why such feelings occur. In fact, the new science of consciousness makes an enormous use of purely subjective phenomena, such as visual illusions, misperceived pictures, psychiatric delusions, and other figments of the imagination. Only these events allow us to distinguish objective physical stimulation from subjective perception, and therefore to search for brain correlates of the latter rather than the former. As consciousness scientists, we are never as pleased as when we discover a new visual display that can be subjectively either seen or missed, or a sound that is sometimes reported as audible and sometimes as inaudible. As long as we carefully record, on every trial, what our participants feel, we are in business, because then we can sort the trials into conscious and unconscious ones and search for brain activity patterns that separate them.”
As I have discussed earlier, OBEs are complex phenomena which are hard to attack. Fortunately, the framework provided by Crick & Koch (1995) gives a more feasible way of studying the neural correlates of consciousness described by Dehaene’s quote. This framework assumes as first stage of the research program a vast inventory of multiple visual codes and visual brain structures. The goal then becomes to establish which ones contribute to reportability and how (i.e., the precise conditions). With these assumptions and goals in mind, neuropsychological syndromes that involve parts of the visual system are our best bets.
The phenomenon of blindsight is an especially good example of the visual cortex’s involvement in conscious reports. Blindsight is usually associated with visual scotoma (lack of vision in a sector) secondary to a lesion in V1. Individuals with this condition report no consciousness of a visual stimulus flashed within their scotoma. Yet, when forced to give an answer, these individuals perform significantly better than chance in many perceptual tasks. The mechanism that sends information to higher levels of processing yet bypasses centers that consciously detect such information is presumably an “indirect” pathway. It presumably goes from the superior colliculus (key for orienting eye movements and directing action to a goal), then inputs to ventral and dorsal pathways that bypass V1. Importantly, a mechanism extends to emotional subliminal perception bypassing V1 via the amygdala. However, V1 is not the only critical connection. Further in the sequence of processing, beyond the extrastriate areas, lesions in the ventral visual pathway can lead to visual form agnosia. The neurological case of D.F., studied by Goodale and colleagues, shows that impairment of this pathway causes extreme agnosia for common objects, geometric forms and line orientation. In contrast, D.F.’s dorsal visual pathway was intact and functioning normally. Thus, she was unable to point the mail slot of a mailbox but able to post a letter into it. A classic interpretation of this case study is that the ventral pathway supports phenomenal consciousness, whereas the dorsal one operates unconsciously.
Support for the division between the two pathways comes from the study of another neuropsychological syndrome of dorsal pathway impairment. Optic ataxia is a lack of coordination between visual inputs and hand movements, resulting in the inability to reach and grab objects. When the dorsal pathway is damaged but V1 and the ventral pathway are intact, as in I.G.’s case, calibrating correctly then pointing to a jumping target is done with a very slow, conscious and strategic effort. In normal people, this is done as if on autopilot and controlled by the dorsal pathway. However, if the correction for pointing correctly at the target stimulus is inhibited at onset, before the trial actually starts starting (by for example delaying or disturbing the perception of the target or the response), I.G. performs much better than normal controls.
Another state that shows the key role of the ventral pathway in consciousness is Charles-Bonnet syndrome. People who suffer from it have chronic hallucinations as a result of vision loss, but are conscious that their hallucinations are not real. Neuroimaging studies of such episodes in Charles-Bonnet patients show increased CBF in ventral visual areas for conscious perception of the same contents seen in the hallucinations (faces, colour, texture, etc).
Therefore, one conclusion that could be drawn from these neuropsychological syndromes of the visual system is that conscious reportability seems linked with ventral object-processing pathways of the visual system. However, the “background” unconscious processing occurs in the dorsal action-location processing pathway of the visual system. Are there necessary conditions for information in the ventral pathway to be conscious? In other words, are we necessarily aware of all the information in the ventral pathway, or does a portion of unconscious processing also occur in there?
We have already encountered a neuropsychological syndrome called unilateral spatial neglect. In this syndrome, the ventral pathway is intact but attentional functions in the ventral system are impaired. Neglect is defined as the inability to respond, perceive or represent stimuli on the side contralateral to the lesion. Most neglect patients have impairment in the right dorsal pathway which involves input to or from the parietal cortex within what is known as the spatial attention network. Significant evidence shows that the ventral system represents neglected information; what lacks is the “gating” or “amplification” from the attention network to make this information consciously available. In other words, top-down attention can amplify information. This is also obvious in unconscious automatic processing. The temporal window of attention influences unconscious priming for masked stimuli. For example, cuing attention to the scotoma where a target is going to appear improves performance even without conscious perception. Other evidence shows that the prime-target effect on subsequent tasks where some of the previously presented information needs to be compared is facilitated (speeded up) by the attentional window. If attention is not deployed at the narrow time window when prime and target are presented in succession temporally close to each other then all priming effects disappear.
The opposite, however, occurs when attentional amplification occurs and the base knowledge content lacks. In these cases, interpretative-fictional processes are triggered in visual consciousness to fill in the missing information. This is the case of visual completeness reported in normal people in spite of the poverty of perception and our blind spots. In Capgras syndrome, a rare clinical situation where patients recognize the faces of familiar individuals but claim that the person is a look-alike impostor. Capgras patients recognize faces but do not have an associated emotional response, thus rationalizing it as an impostor. Similar interpretations occur in split-brain patients similar to anosognosia.
A theory has recently been proposed to group these phenomena under one big umbrella, the global neuronal workspace (GNW). This theory asserts that many local and isolated networks are active in parallel and process information unconsciously in both ventral and dorsal pathways. However, when one of these networks is also engaged by attentional amplification, a global brain-scale state of coherent activity arises – this is a neuronal workspace of ongoing activity. In this workspace, which can span the whole brain, information becomes simultaneously available for many processes and to many networks. This “global availability” of information through the workspace is the subjective experience of a conscious state. As a result, some processes remain locally segregated and do not progress to the connection to the global workspace. Therefore, they do not benefit from attentional amplification and remain unconscious. In other cases such as neglect, attentional failure does not engage the global workspace. Some information which could pass the threshold of consciousness cannot be shared globally but remains globally available to some networks. Finally, some unconscious processes may benefit from the preparatory conscious setting and from the effect of attentional amplification, possibly eventually becoming conscious. These processes can be better thought of as preconscious. It is easy to see how GNW, Information Integration Theory and the functional connectome framework all explain consciousness similarly, a global brain state that is essential for high level, difficult and time consuming mental tasks that cannot be automated.
6.7 Drugs and altered states of consciousness
Psychoactive drugs are classified in 4 categories based on their verbally reported effects on consciousness (phenomenology).
- The Low (Downers); Sedatives & hypnotics, their action decreases the brain’s metabolism and/or increases GABA activity. They are typically relaxing, inhibiting, mentally slowing or analgesics. Common examples of these drugs are tranquilizers, such as Valium. Note that marijuana (Cannabis sativa) is not part of this category, since it enhances some sensations and emotions.
- The High (Stimulants); their main effect is euphoria. Common examples are caffeine, nicotine/tobacco and amphetamines, though the most popular is cocaine (and its purified form, crack). Cocaine’s blocking of dopamine reuptake leads to powerful (and addictive) effects. Taking amphetamines intravenously is termed speed, whereas taking amphetamines and opioids is called a speedball.
- The Rush (Opioids); taken intravenously, these drugs – especially heroin and its derivatives- cause a sublime “rush” (euphoria and analgesia). Natural compounds were derived from opium, leading to morphine and codeine, but were refined and synthesized further into semi-synthetic heroin to fully synthetic methadone and Demerol (originally made for pain management). Ironically enough, heroin was synthesized by researchers looking for a less addictive version of morphine.
- The Far Out (Hallucinogens/Psychedelics); natural (mescaline) and synthetic (LSD), these drugs usually cause heightened visual sensations and hallucinations. Perhaps unexpectedly, they are usually unharmful even in large doses. Very few similarities exist between them, except that a different variety of each exists for almost each neurotransmitter. For example, cholinergic varieties include scopolamine (harmful), serotonergic ones LSD and psilocybin, and MDMA/mescaline for norepinephrinergic ones.
6.7.1 Ego dissolution
There is a lot of heterogeneity and variety of phenomenological experiences associated with psychedelics and other drugs, and it is impossible to draw simple commonalities. However, one experience which is associated with psychedelics – and to which many other drugs can lead to at very high dosage, with peril of addiction and overdose – is ego dissolution. It has been described in many ways; “dissolving in the universal ocean”, “merging with the almighty”, “becoming one with the void”… Ego dissolution has many spiritual interpretations and beliefs associated with it, historically and culturally, as a mind expanding, higher experience.
But, are drug-induced altered states truly higher states of consciousness? Some have posited them to be simply transient hypofrontality, whereas others have put ego in the center. To get a quick overview of two different opinions on the topic, watch Arne Dietrich (https://www.youtube.com/watch?v=syfalikXBLA) and Tom Metzinger (https://www.youtube.com/watch?v=5ZsDDseI5QI) explain themselves.
6.7.2 Lysergic acid diethylamide (LSD) and ego dissolution
LSD alters the organization of resting-state networks. Tagliazucchi et al. (2016) found that ego dissolution induced by LSD correlated with increased global functional connectivity; these increases resulted from a breakdown in the integrity of resting-state networks. Here, the default-mode network (DMN) and SLN were both affected. Alterations of DMN induced by LSD also reduced mental time travel.
Drugs unbind aspects of the self-model by altering the functional connectivity of Large State networks. In other words:
- Ego dissolution experiments reveal that the self-model plays an important binding function in consciousness and cognitive processes, allowing us to have the perception of a unitary consciousness
- However, ego dissolution reflects an experience that the self does not exist if not as a perception, resulting from the complex process hypothesized by Tom Metzinger. (Letheby & Gerrans, 2017)