Module 1.1 Promoting Good Health and Wellness
Learning Objectives
- Explain good dental hygiene practices in early learning and child care programs.
- Discuss the importance of sleep.
- Identify different screenings early learning and child care programs can implement.
- Relate the importance of developmental screening.
- Review ways to engage families in the screening process.
Introduction
Healthy development continues to support learning throughout childhood and later life. Early learning and childcare programs can support children’s oral health and healthy sleep habits. And they can help identify developmental and health concerns with screening.

Dental Hygiene
Dental hygiene is important to prevent Early Childhood Caries (ECC), which is a term used to describe tooth decay, including filled or extracted teeth due to decay, in the primary teeth (baby teeth). It is important to rethink the way we “treat” dental caries. Traditionally, we would wait until a child had a cavity and “treat” the cavity with a filling. To prevent ECC, we must intervene before the first cavity develops. Early learning and child care programs can teach children and families about dental hygiene and oral care as well as implement good dental hygiene practices. Here are some ideas:
- Use teaching practices that engage children and promoting thinking critically. Consider asking questions such as:
- How do you brush your teeth?
- Why do you brush your teeth?
- What else can you do to keep your mouth and teeth healthy?
- What happens if you don’t brush your teeth?
- Tell me about your last visit to the dentist
- Integrate oral health into activities (in addition to tooth brushing). Some possibilities include:
- Having children separate pictures of foods that are good for oral health from pictures of foods that are high in sugar.
- Reading books with positive oral health messages to children.
- Having children pretend they are visiting a dental office.
- Singing songs about oral health.
- Engage families in promoting oral health at home. Some ways to do this include:
- Working with families to find the best ways to position their child for tooth brushing. Remind families that young children cannot brush their teeth well until age 7 to 8. It is also important for a parent to brush their child’s teeth or help them with brushing.
- Asking families to take photographs of their child brushing their teeth and helping the child write stories about their experience.
- Helping families choose and prepare foods that promote good oral health.
- Encouraging families to ask their child what they learned about oral health in school that day.
- Offering families suggestions for at-home activities that support what children are learning about oral health at school.
Classroom Tooth Brushing Steps
- Sitting at a table in a circle, children brush teeth as a group activity every day.
- Give each child a small paper cup, a paper towel, and a soft-bristled, child-sized toothbrush.
- Put a small (pea-sized) dab of fluoride toothpaste on the inside rim of each cup, and have children use their toothbrushes to pick up the dabs of toothpaste.
- Brush together for two minutes, using an egg timer or a song that lasts for about two minutes.
- Brush your teeth with the children to set an example, and remind them to brush all of their teeth, on all sides.
- When the two minutes are up, have the children spit any extra toothpaste into their cups, wipe their mouths and throw the cups and paper towels away.
- Children can go to the sink in groups to rinse their toothbrushes and put the toothbrushes in holders to dry 319 that separate each brush from touching.

Sleep Hygiene
It’s important to get enough sleep. Sleep supports mind and body health and growth. Getting enough sleep isn’t only about total hours of sleep. It’s also important to get good quality sleep on a regular schedule to feel rested upon waking.
- Sleep is an important part of life! Young children spend around half of their time asleep (American Psychological Association, n.d.).
- Infants need to sleep between 12 and 16 hours a day (including naps).
- Toddlers need to sleep between 11 and 14 hours a day (including naps).
- Preschoolers need to sleep between 10 and 13 hours a day (including naps).
- School-aged children need 9 to 12 hours of sleep each night.
We know how busy they are when they are awake, but what are they doing during all of those restful hours? Sleep has many purposes.
- Growth: Growth hormone is released when children sleep. Young children are growing in their sleep, and since they have a lot of growing to do, they need all the sleep they can get.
- Restoration: Some sleep researchers have found that sleep is important for letting the brain relax and restore some of the hormones and nutrients it needs.
- Memory: Sleep is also a time when the brain is figuring out what experiences from the day are important to remember.
- Health: One study found that infants and toddlers need at least 12 hours of sleep in a 24-hour day. When infants and toddlers had less than 12 hours, they were more likely to be obese by the age of 3 (Taveras et. al. 2008).
The Culture of Sleep and Early Learning and Childcare Programs
Across the world people sleep in different ways. Some people sleep inside, some sleep outside. Some people sleep in beds, others in hammocks or on mats on the floor. Some people sleep alone, some sleep with a spouse or children or both. Some people sleep only at night, while others value a nap during the day. How, when, and where people choose to sleep has a lot to do with their culture, traditions, and customs. This can include where they live, how their family sleeps, even how many bedrooms are in their home. Educators have a role in providing a sleep environment that is comfortable and safe for the children in their care, while honoring families’ cultural beliefs.
What can educators do to help young children feel more “at home” when it is time for them to rest?
- Think of sleep and sleep routines as part of the child’s individualized curriculum.
- Educators should meet with a family before a child enters your care. This is an opportunity to find out about a child’s sleep habits before they join the classroom. When you know how a baby sleeps at home, you can use that information to plan for how they might sleep best in your care.
- Brainstorm ways to adapt your learning environment to help a child feel “at home” during rest times. For example, an infant who is used to sleeping in a busy environment might nap better if you roll a crib into the playroom. Some mobile infants and toddlers might have a hard time sleeping because they think they will miss something fun! These children benefit from having a very quiet place to fall asleep. When you have a positive relationship with a baby it will be easier to know what will help them relax into sleep.
- Encourage families to bring in “a little bit of home” to the program – like a stuffed animal or special blanket, some sleep better with ‘weight’ on them. A comfort item from home can help children feel connected to their families. They might want that comfort all day. The comfort item from home can also help children make the transition to sleep while in your care. Make sure that infants under one year of age do not have any extra toys or blankets in the crib with them.
- Share with families what you learn about their child. Use pick-up, drop-off times and your app to ask questions about sleep at home. Families can share information that could make their child more comfortable in your care. You can be a resource for families about sleep and their child. Remember that families are the experts about their child.
Indigenous Perspective
In certain Indigenous cultures, it is believed that babies have a direct link to the creator through their soft spot on their heads. This is viewed as a direct link from the physical world to the Skyworld. After a baby’s soft spot closes, they begin to connect to the Skyworld through dreams.
A baby’s soft spot on their head is a physical sign of interconnectedness.
Napping and Individual Differences
Have you noticed that some children will fall asleep every day at the same time no matter what else is going on? These children could fall asleep into their lunch if it is served too late! Have you known children who seem to fall asleep easily some days and other times just can’t settle into sleep? These children might need a very stable routine. Some toddlers nap less and sleep more at night while others need to have a long sleep during the day.
Temperament and Sleep
Some of the different patterns in children’s sleep has to do with their temperament. Temperament is like the personality we are born with. Some children are naturally easy-going and adapt to new situations while others really need a routine that is the same every day. One child might fall asleep easily just by putting her in her crib or cot when she is drifting off to sleep. Another child might fall asleep in your arms, but startle awake the moment they realize they have been laid down alone.
Circadian Rhythms and Sleep
Something else that can make nap time easy or difficult for young children has to do with their natural sleep cycles. Everyone has a kind of “clock” inside of their bodies that tells them when they are hungry or sleepy. The cycle of this clock is called circadian rhythms. Circadian rhythms are the patterns of sleeping, waking, eating, body temperature and even hormone releases in your body over a twenty-four-hour period. How much children need to sleep, when they feel tired, and how easily they can fall asleep are all related to their circadian rhythms.
Meeting Each Individual Child’s Sleep Needs
Thinking about the circadian rhythms and temperament reminds us how each child is different. That is why it is important to have nap times that meet the needs of all children in your care. Helping young children to learn to recognize their bodies’ needs and find ways to meet those needs is the very important skill of self-regulation.

Individualizing Nap Schedules
Creating a space for sleepy children can allow them to relax or nap when their body tells them they are tired. It can take some creativity to figure out how to let a young child nap or rest when they are tired.
What do you do if a child won’t nap when others are? How does one child rest quietly in a busy classroom?
Two-and-a-half-year-old Henry is new to your classroom. His mother has shared with you that he does not nap during the day with her. When nap time comes around you can tell that Henry does not seem very tired.
What can you do for Henry, or other children like him, while the rest of the class sleeps?
- Do you have a “cozy corner” that could also be a one child nap area?
- Are there soft places to sit and relax with a book or stuffed animal?
- Are books or other quiet activities provided if a child can’t rest or settle when other children are?
- Are children provided techniques and strategies for calming their bodies e.g., deep breathing, tensing and relaxing their bodies, feeling their heartbeat, etc.? 326
33.1 (1) Every licensee shall ensure that a child who is younger than 12 months who receives childcare at a childcare centre it operates or at a premises where it oversees the provision of home childcare is placed for sleep in a manner consistent with the recommendations set out in the document entitled “Joint Statement on Safe Sleep: Preventing Sudden Infant Deaths in Canada”, published by the Public Health Agency of Canada, as amended from time to time, unless the child’s physician recommends otherwise in writing. O. Reg. 126/16, s. 23.
(2) Every licensee shall ensure that, if childcare is provided for a child who regularly sleeps at a childcare centre the licensee operates or at a premises where it oversees the provision of home childcare,
(a) an employee or the home childcare provider periodically performs a direct visual check of each sleeping child who is in a licensed infant or toddler age group, is in a licensed family age group and is younger than 24 months, or is at a home childcare premises and is younger than 24 months, by being physically present beside the child while the child is sleeping and looking for indicators of distress or unusual behaviours;
(b) there is sufficient light in the sleeping area or room to conduct direct visual checks; and
(c) there are written policies and procedures at the childcare centre or home childcare premises with respect to sleep, and the policies and procedures,
(i) provide that children will be assigned to individual cribs or cots in accordance with this Regulation,
(ii) provide that parents will be consulted respecting a child’s sleeping arrangements at the time the child is enrolled and at any other appropriate time, such as at transitions between programs or rooms or upon a parent’s request,
(iii) provide that parents of children younger than 12 months will be advised of the licensee’s obligation under subsection (1),
(iv) provide that parents of children who regularly sleep at the childcare centre or home childcare premises will be advised of the centre’s or agency’s policies and procedures regarding children’s sleep,
(v) provide that the observance of any significant changes in a child’s sleeping patterns or behaviours during sleep will be communicated to parents and will result in adjustments to the manner in which the child is supervised during sleep, and
(vi) include details regarding the performance of direct visual checks, including how frequently direct visual checks will be performed and how direct visual checks will be documented. O. Reg. 126/16, s. 23; O. Reg. 174/21, s. 19.
(3) In determining the matters described in clause (2) (c) (vi) in respect of children who are enrolled with a home childcare agency and who receive childcare at a home childcare premises, the licensee shall consider parents’ input, the sleep environment at the premises and the proximity of the sleeping area or room to the childcare provider when the child is sleeping. O. Reg. 126/16, s. 23.
(4) Every licensee shall ensure that in each childcare centre it operates that has a separate area or room for sleeping, there is a system in place to immediately identify which children are present in the area or room. O. Reg. 126/16, s. 23.
(5) Every licensee shall ensure that if electronic sleep monitoring devices are used at a childcare centre it operates or at a premises where it oversees the provision of home childcare,
(a) each electronic sleep monitoring device is able to detect and monitor the sounds and, if applicable, video images, of every sleeping child;
(b) the receiver unit of the electronic sleep monitoring device is actively monitored by employees at the childcare centre or the home childcare provider at all times;
(c) each electronic sleep monitoring device is checked daily to ensure it is functioning properly; and
(d) electronic sleep monitoring devices are not used as a replacement for the direct visual checks required under clause (2) (a). O. Reg. 126/16, s. 23. (O. Reg. 137/15: General)
Developmental and Health Screenings
There are specific health conditions that impact learning and development, which can be identified and treated early. These conditions can often be identified through early health screening.
Screening is the first step in getting to know a child at the beginning of each enrollment year. This “baseline data” helps staff plan and individualize services. It also helps them identify “red flags” for further examination or evaluation. When concerns go unidentified, they can lead to bigger problems.
Screening helps staff and families:
- Celebrate milestones: Every family looks forward to seeing a child’s first smile, first step, and first words. Regular screenings with early childhood professionals help raise awareness of a child’s development, making it easier to celebrate developmental milestones.
- Promote universal screening: All children need support in the early years to stay healthy and happy. Just like regular hearing and vision screenings can assure that children are able to hear and see clearly, developmental and behavioral screenings can assure that children are making progress in areas such as language, social, or motor development.
- Identify possible delays and concerns early: With regular screenings, families, educators, and other professionals can assure that young children get the services and supports they need as early as possible to help them thrive.
- Enhance developmental supports: Families are children’s first and most important teachers. Tools, guidance, and tips recommended by experts, can help families support their children’s development.
Screening is part of a larger process professionals use to learn about children’s health and development. In partnership with families, developmental monitoring (or surveillance), screening, and assessment keep children on track developmentally.
What is the Difference Between Screening, Assessment, and Evaluation
Screening
The screening process is the preliminary step to determine if sensory, behavioral, and development skills are progressing as expected. The screening itself does not determine a diagnosis or need for early intervention. Educators, families and professionals can implement screening.
Assessment
Assessment is an on-going process to determine a child’s and family’s strengths and needs. The assessment process should be continued throughout a child’s eligibility and be used to determine strategies to support the development of the child in the classroom and at home. This can be either a formal or informal process. Educators and professionals would do this informally through observations. Only professionals licensed to complete an assessment would do so formally.
Evaluation
An evaluation is performed by a qualified professional to identify or diagnose a developmental, sensory, or behavioral condition or disability requiring intervention. Only children who were identified through screening and ongoing assessment as possibly having a condition or disability might require intervention
Important things to remember about screening:
- Children develop rapidly during the first three years of life, so keeping a watchful eye on health and development for infants and toddlers is critical.
- Most early childhood programs serve diverse families. Therefore, the best screening tools gather information in ways that respond to culture and language.
- Developmental screening using research-based standardized developmental screening instruments that are valid and reliable for the population and purpose for which they will be used; age, developmentally, culturally, and linguistically appropriate, and appropriate for children with disabilities, as needed; and conducted by qualified and trained personnel.
Engaging Families in Screening and Follow-Up
Families can be your most powerful ally and asset throughout the screening process. They are the expert on their child and can provide meaningful and reliable information. Screenings are also an opportunity to support families to focus on their child and increase their understanding of their child’s development.
When families are active partners in the assessment (and intervention) process, educators and families can share an understanding of what is best for the child, the families ‘ priorities, and goals for the child’s learning and development.
Engaging Families
Educators can engage families by:
- Discussing and explaining the screening process and results.
- Make sure to include an explanation of the tools you used, and any relevant developmental, linguistic or cultural accommodations made for their child.
- Listening to parent feedback and concerns on the screening and assessment system.
- What was useful or confusing to them?
- Helping families navigate follow up.
- Does the child need a formal evaluation? If so, how can you help the parent begin this process?
- Partnering with families to determine individual health services appropriate for their child.
Developmental Monitoring and Screening
The first years of life are so important for a child’s development. Early experiences make a difference in how young children’s brains develop and can influence lifelong learning and health. Early childhood educators spend a great deal of time with young children and are instrumental in determining many of the kinds of experiences they will have. Developmental monitoring means observing and noting specific ways a child plays, learns, speaks, acts, and moves every day, in an ongoing way. Developmental monitoring often involves tracking a child’s development using a checklist of developmental milestones.
Educators are in a unique position to monitor the development of each child in their care. They may be the first one to observe potential delays in a child’s development. Working with groups of same-aged children can help educators recognize children who reach milestones early and late. Working with children of different ages can help educators notice if a child’s skills are more similar to those of a younger or older child than to those of his or her same-aged peers. Because educators spend their day teaching, playing with, and watching children, they may find themselves concerned that a child in their care is not reaching milestones that other children his or her age have, or they may have families ask them if they are concerned about their child’s development.
“The first time I heard the term “developmental monitoring,” I was really intimidated and thought, “this sounds really complicated and time-consuming. How am I going to do that on top of everything else I have to do during the day?”
I was so relieved when I found out that “developmental monitoring” is just a fancy way of saying “watch, observe and record what the kids are doing to make sure they’re on track.” I just mark on a simple checklist when children meet milestones.
We observe children every day anyway. We watch what they’re doing when they play in the classroom or outside, when they eat, and so on. Monitoring is just that: watching and observing and recording what you see. Making a check on a list when a child meets a milestone takes about two seconds, and it’s easier than just about anything else we do all day. It’s definitely easier than getting a room full of toddlers to sleep at naptime, and it’s a lot more fun than changing diapers!
And if that’s all it takes to really make sure each child is on track and to make sure I’m not missing anything in all the hubbub each day, I’m all over it!”
-Ms. Carolyn (an early childhood educator)
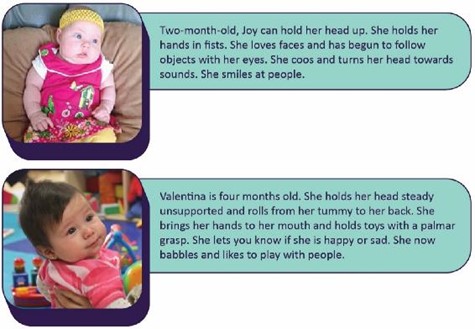
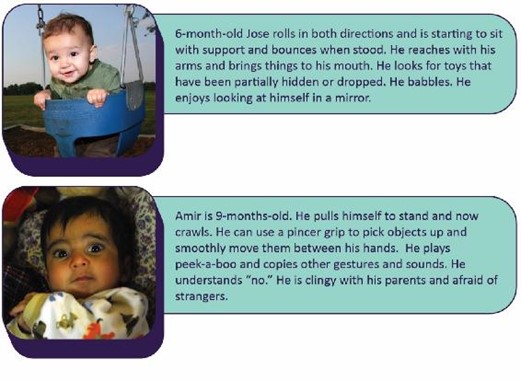
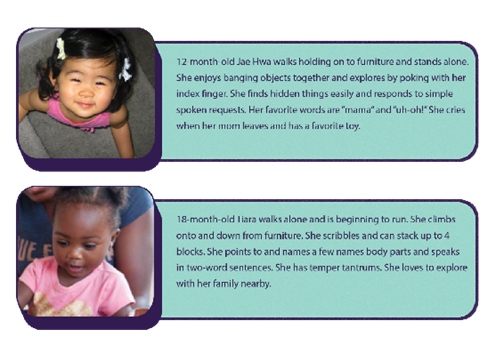
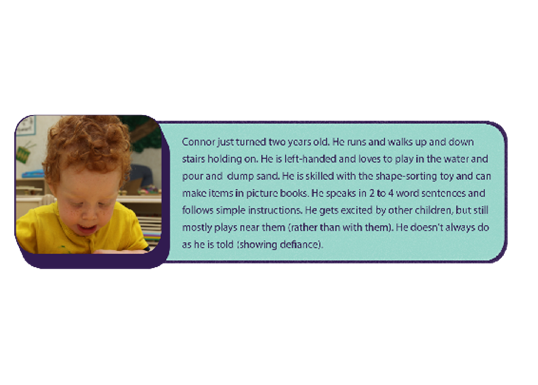
Here are some examples of children birth to age 5 that display typical skills for their age:
Pause to Reflect 💭
Do you feel you are less knowledgeable about or have less experience with a specific age of children?
What can you do to improve your familiarity with the skills typically achieved for children that age? Why would this be important?
Developmental screening is a more formal process that uses a validated screening tool at specific ages to determine if a child’s development is on track or whether he or she needs to be referred for further evaluation.
Screening alone is not enough to identify a developmental concern. Rather, it helps educators and families decide whether to refer a child for more evaluation by a qualified professional. The earlier a possible delay is identified, the earlier a program can refer a child for further evaluation and additional supports and services.
Most children with developmental delays are not identified early enough for them to benefit from early intervention services; early learning and childcare programs can help change that. Although about 1 in 6 children has a developmental disability, less than half of these children are identified as having a problem before starting school. Too often, adults don’t recognize the signs of a potential developmental disability, they are not sure if their concern is warranted, or they don’t have resources to help make their concern easier to talk about. But pinpointing concerns and talking about them is very important to get a child the help he or she might need.
Developmental screening involves:
- Research-based, standardized developmental screening tools.
- Information from family members, educators, and other professionals who know the child.
- Written parental consent before starting the screening.
- Communication with families in their home language.
Appropriate Screening Tools
When searching for screening tools, keep the following in mind.
- Screening tools must be research-based and designed to be a brief measure of development that identifies if the child needs a more in-depth evaluation.
- Screening tools should be:
- Age-appropriate
- Culturally appropriate
- Sensitive to the family’s home language
- Used by trained and qualified personnel
- Valid for the intended results
- Reliable across users
- Clearly identified for use in screening
Programs need to make careful and informed decisions about whether to screen a child who is a dual language learner (DLL) in their home language, English, or both. Some skills may look different depending on the child’s culture and background. Use a screening tool that considers the child’s cultural context. When a culturally appropriate screening tool is not available, asking families about their child’s typical behavior becomes even more critical. This information helps professionals interpret screening results.
Some currently used in Canada include:
- Ages and Stages Questionnaires (ASQ)
- Nipissing District Developmental Screen (NDDS)
- Receptive, Expressive, Emergent Language Test (REEL-3)
- Communication and Symbolic Behavior Scales (CSBS)
- Parent’s Evaluation of Development Status (PEDS)
- Modified Checklist for Autism in Toddlers (M-CHAT)
- Screening Tool for Autism in Toddlers and Young Children (STAT)
Timing
Programs should complete the first developmental screening in the first month or two of care. Programs may keep track of a child’s development with an annual screening after that. Also, a child and family’s primary health care provider may do developmental screening, autism spectrum disorder screening, and developmental surveillance.
After Screening
These are examples of the next steps a program might take based on the results of the screening:
- Results: There are no concerns.
Action: The child participates in ongoing, individualized care. Educators do ongoing child assessments. - Results: The results are unclear or there may be additional concerns.
Action: The child participates in ongoing, individualized care. Educators do ongoing child assessments. The family and educators closely observe the child’s development over time to decide if they should re-screen or evaluate the child. - Results: The screening or information collected from family members, teachers, and other program staff found some concerns.
Action: The child participates in ongoing, individualized care. Educators work with the family to refer the child for further evaluation. Families may need support to navigate the referral and evaluation process.
If a delay or disability is diagnosed, early treatment is important.
Vision Screening
Families and educators cannot always tell when a child has trouble seeing. Observation alone isn’t enough. This is why implementing evidence-based vision screening throughout early childhood is important.
Timely vision screening (coupled with an eye examination when indicated) is an important step toward early detection of any possible vision problems. Early detection can lead to an effective intervention and help to restore proper vision. Young children rarely complain when they can’t see well because to them, it’s normal.
Engaging Families
It is easier for families to partner with educators and health care providers when they understand how vision influences their child’s development and learning. Preparing families about what to expect from a vision screening helps them know how to prepare their child. It is also important to talk about who will have access to their child’s screening results. One of the best ways to promote children’s vision health is by developing and implementing policies and procedures that both define and support ways for educators to collaborate with families.
Include questions on the program’s family health history form to identify children who may have a higher risk of vision problems. For example, is there a family history of amblyopia, strabismus, or early and serious eye disease? Provide resources to help families learn more about healthy eyes and the importance of early detection of vision problems. Do families know that it isn’t always possible to tell if children have a vision problem just by looking at their eyes? Or that young children seldom complain when they can’t see well?
In addition to assuring timely vision screening, programs can support children and families who have been given treatment recommendations from an eye specialist (such as wearing glasses or patching one eye for amblyopia), as well as reminding families of follow-up visits to the eye doctor whenever recommended.

Rescreeningbaby hearing
Programs that perform vision screenings will need to determine when to rescreen children who do not pass. Some children may be unable to pay attention, cooperate or understand what they need to do during the first attempt at screening. This is especially true for visual acuity testing. These children may not have “failed” their vision screening. They may be considered “untestable.” Research shows that preschool children who are “untestable” are almost twice as likely to have a vision problem as those who successfully pass a screening. They should be rescreened as soon as possible, but not longer than 6 months later. If a child fails or is untestable at the second attempt, consider referring the child for a full eye examination.
Ongoing Care
It is important to remember that screening only provides a vision assessment at one moment in time. Occasionally a family member or educator will identify a new or different vision concern after a child has been previously screened. In addition, as children grow their eyes change and new signs of an eye problem or blurred vision can arise as they mature. Programs should address this new concern with the parent and the health care provider promptly.
Hearing Screening
Families and educators cannot always tell when a child is deaf or hard of hearing. Observation of failing to respond to sounds and delay in speech alone, isn’t enough. This is why implementing evidence-based hearing screening throughout early childhood is important.
Hearing helps us communicate with others and understand the world around us. In Canada, hearing loss is the most common congenital condition (meaning it is present at birth). About 3 in 1000 babies are born severely deaf. And another 3 in 1000 have serious hearing loss (Canadian Paediatric Society).
A child may also experience a decline in hearing ability at any time caused by illness, physical trauma, or environmental or genetic factors. It is estimated that the incidence of permanent hearing loss doubles by the time children enter school. A child may have difficulty hearing in one ear or both ears. The difficulty may be temporary or permanent. It may be mild, or it may be a complete inability to hear spoken language and other important sounds.
Any inability to hear clearly can get in the way of a child’s speech, language, social and emotional development, and school readiness. Intervention may improve social and emotional and academic achievement when children who are deaf or hard of hearing are identified early.

An evidence-based hearing screening is a way to identify children who need an evaluation to determine if they are deaf or hard of hearing. Prior to discharge from the hospital, almost all newborns are screened, and an evaluation is necessary for those who do not pass the screening. In Ontario, infant hearing screening can be accessed through EarlyON or local Health Units.
Engaging Families
It is easier for families to partner with educators and health care providers when they understand how hearing influences their child’s speech and language development, socialization, and learning. Preparing families about what to expect from a hearing screening helps them know how to prepare their child. It is also important to talk about who will have access to their child’s screening results. When a child does not pass a hearing screening, programs can provide support to help families follow up with referrals and any recommended treatment. If a child is identified as deaf or hard of hearing, collaboration between the family, the early learning and childcare program, and the child’s audiologist and other early intervention providers will be helpful. Share information with the family about the importance of hearing for children’s language development and communication. This supports a family’s health literacy, and it may help them complete the follow-up steps.
Rescreening
If your program performs a hearing screening and a child does not pass, it is important for you to collaborate with and support the family to complete all recommended follow-up steps.
- The child is typically screened a second time within about 2 weeks.
- If the child does not pass, the child should be referred to a health care provider for a middle ear evaluation. A health care provider can diagnose and treat common problems such as earwax buildup or middle ear infections. A third screening is necessary after the medical examination.
- If a child still does not pass, programs should recommend for a referral to a pediatric audiologist for a complete diagnostic evaluation.
It is also important for programs to support families to follow up if the program obtains results from the child’s health care provider indicating that the child did not pass a hearing screening.
Pause to Reflect 💭
Do you remember getting your vision or hearing screen during your childhood?
If you were diagnosed with vision or hearing impairments, how was it discovered? At what age did that happen?
Lead Screening
Lead screening measures the level of lead in the blood. According to the Canadian Paediatric Society, lead is a chemical for which there is no safe threshold (Canadian Paediatric Society, 2019). Lead is a poison that is very dangerous for young children because of their small size and rapid growth and development. It can cause anemia, learning difficulties, and other medical problems.
Children can inhale or swallow lead through exposure to:
- Home or childcare environments, including those:
- Built before 1960 with peeling paint or renovation
- Located near a highway or lead industry
- Family members who work with lead or have been treated for lead poisoning
- Imported ceramic pottery for cooking, storing, or serving food
- Home remedies with lead
- Certain candies, which may contain high levels of lead in the wrapper or stick. Be cautious when providing imported candies to children
- Eating paint chips or dirt
- Water pumped through lead-based pipes
Lead screening involves a blood lead test, from a finger stick or a venous blood draw. It is recommended at 12 months and 24 months of age. Children from 3 to 6 years of age should have their blood tested if they missed the 12–24-month test.
Symptoms of Lead Poisoning
Most children with lead poisoning show no symptoms. However, you might notice:
- Developmental delay
- Learning Difficulties
- Irritability
- Headaches
- Poor appetite or stomach-ache
- Weight loss
- Fatigue and sluggishness
- Slow growth and development
- Vomiting
- Constipation
- Hearing loss
Follow-Up to Lead Screening
Buka and Hervouet-Zeiber (2019), in their paper titled “Lead toxicity with a new focus: Addressing low-level lead exposure in Canadian children” state that “Children found to have a BLL (blood lead level) higher than 5 mcg/dL (0.24 mcmol/L) should be investigated thoroughly, and any identified exposure sources should be mitigated as soon as possible.” (Canadian Paediatric Society, 2019).
Lead has negative outcomes on a variety of things, including:
- Attention (easily distracted, challenges with sustained attention, hyperactivity)
- Executive functions (problems with planning, impulse control, flexible thinking, etc.)
- Visual-spatial skills (problems related to visual perception, memory, organization, and reasoning with visually presented information)
- Social behavior (aggression, disruptive behavior, poor self-regulation)
- Speech and language (problems with phonological and sentence processing and spoken word recognition)
- Fine and gross motor skills (unsteadiness, clumsiness, and problems with coordination, visual-motor control, and dexterity)
Depending on the effects of lead poisoning, early learning and childcare programs can implement intervention services to support the child. Other treatments include:
- Nutrition counseling
- Iron supplements
- Medication to remove the lead from the blood
- Follow-up testing of the child’s blood
- Referral for developmental testing
Social and Emotional and Behavioral Screening
Young children are learning to get along with others and manage their own emotions. When a child enters a program, educators get to know what social and emotional skills children are working on. They can use social and emotional or behavioral screening tools to gather that information.
Social and emotional health—the ability to form strong relationships, solve problems, and express and manage emotions—is critical for school readiness and lifelong success. Without it, young children are more likely to:
- Have difficulty experiencing or showing emotions, which may lead to withdrawal from social activities and maintaining distance from others.
- Have trouble making friends and getting along with others.
- Have behaviors, such as biting, hitting, using unkind words, or bullying, behaviors that often lead to difficulty with learning, suspension or expulsion, and later school dropout.
Important Things to Remember
- Brushing or wiping baby teeth with a cloth will start a routine of good dental care.
- Children have independent sleep needs based on their temperament and circadian rhythms.
- Screening is a preliminary step to determine if sensory, behavioral, and development skills are progressing as expected. The screening itself does not determine a diagnosis or need for early intervention. As an educator your role is to inform families of your observations and provide possible next steps.
- Young children rarely complain about not being able to see. Early and regular visions screening can identify issues and effective interventions.
- Lack or loss of hearing can affect development of speech, language and social skills.
- There is no safe level of lead in the blood.
- The ability to form strong relationships, solve problems, and express and manage emotions—is critical for school readiness and lifelong success.
Resources for Further Exploration
Ontario Infant Hearing Program
Lead in Foods, Cosmetics, and Medicines (Centre for Disease Control and Prevention)
References
- American Psychological Association. (n.d.). Resilience Guide for Parents and Teachers. https://www.apa.org/helpcenter/resilience.
- Canadian Paediatric Society. (n.d.). Your baby’s hearing. https://caringforkids.cps.ca/handouts/pregnancy-and-babies/your_babys_hearing#:~:text=Hearing%20loss%20is%20the%20most,1000%20have%20serious%20hearing%20loss.
- Canadian Paediatric Society. (2019). Lead toxicity with a new focus: Addressing low-level lead exposure in Canadian children. https://cps.ca/en/documents/position/lead-toxicity
- Murphey, D., et al. (2014). Are the Children Well? A Model and Recommendations for Promoting the Mental Wellness of the Nation’s Young People. Robert Wood Johnson Foundation. https://www.childtrends.org/wp-content/uploads/2014/07/2014-33AreChildrenWellRWJF.pdf
- O. Reg. 137/15: GENERAL. https://www.ontario.ca/laws/regulation/150137
- Taveras et al (2008). Short Sleep Duration in Infancy and Risk of Childhood Overweight. Arch Pediatr Adolesc Med. 2008;162(4):305-311
