Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
3 Description as a basis for interpretation
This section provides examples of the descriptive features that were covered in the prior sections, and is an introduction to using those descriptive features as a basis for interpreting lesions and inferring the likely pathologic process, cause, pathogenesis and clinical significance. The intent is NOT for you to memorize all these points, but to use them as examples of how descriptive features are used, and can be useful for interpretation. Some of the points covered in this section will be discussed more fully in Systems Pathology (Phase III) and are beyond the scope of this course. Specifically, for the courses in Phase I and II on general pathology, you are not responsible for information on specific diseases. You are only responsible for those points that are relevant to the learning objectives described at the beginning of the notes.
Location of lesions
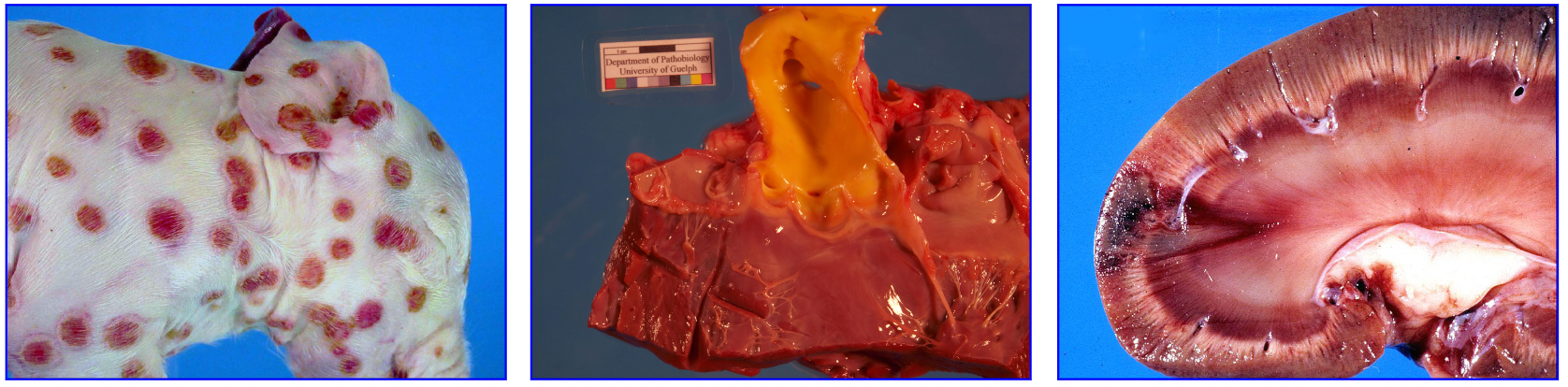
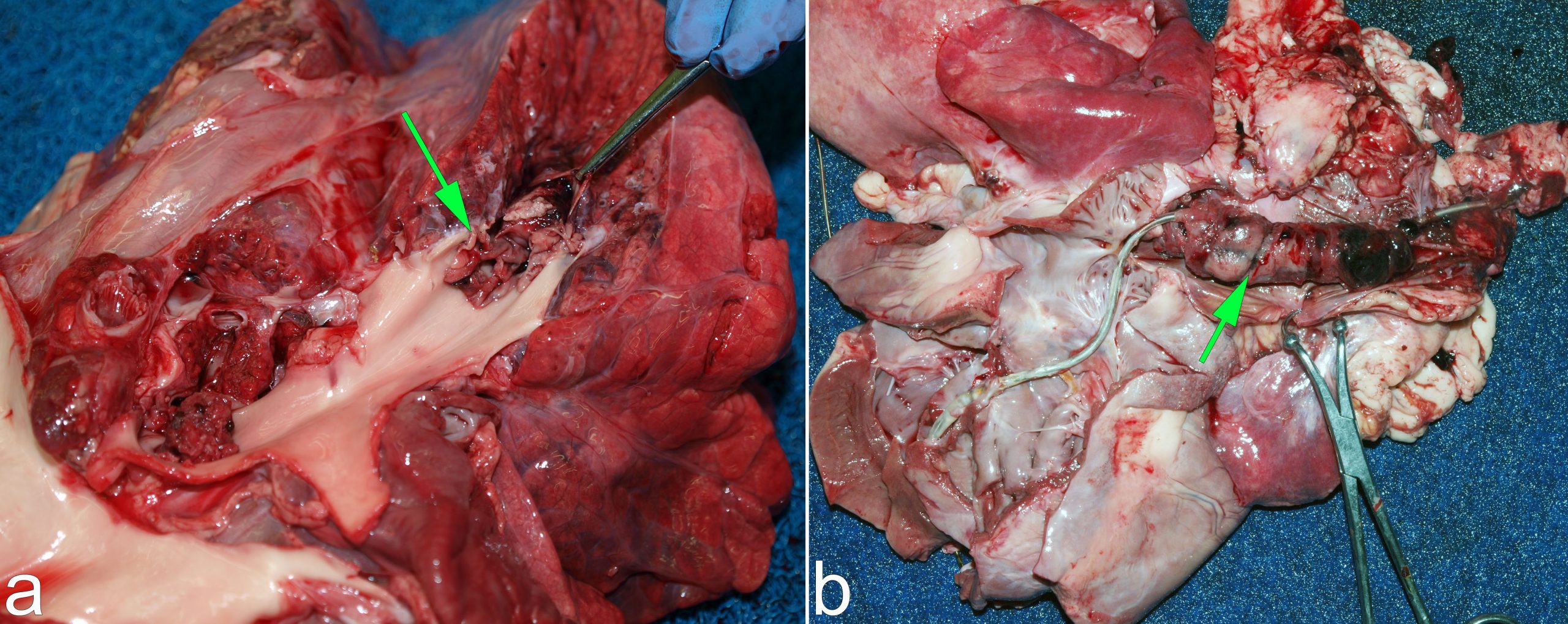
Recognizing that cylindrical structures fill the lumen of blood vessels is critical to identifying them as thrombi. (a) Calf, pulmonary arterial embolism (arrow) from endocarditis of the right atrioventricular valve. (b) Dog, a thrombus (arrow) developed in situ within the cranial vena caval, around a pacemaker lead (the grey wire).
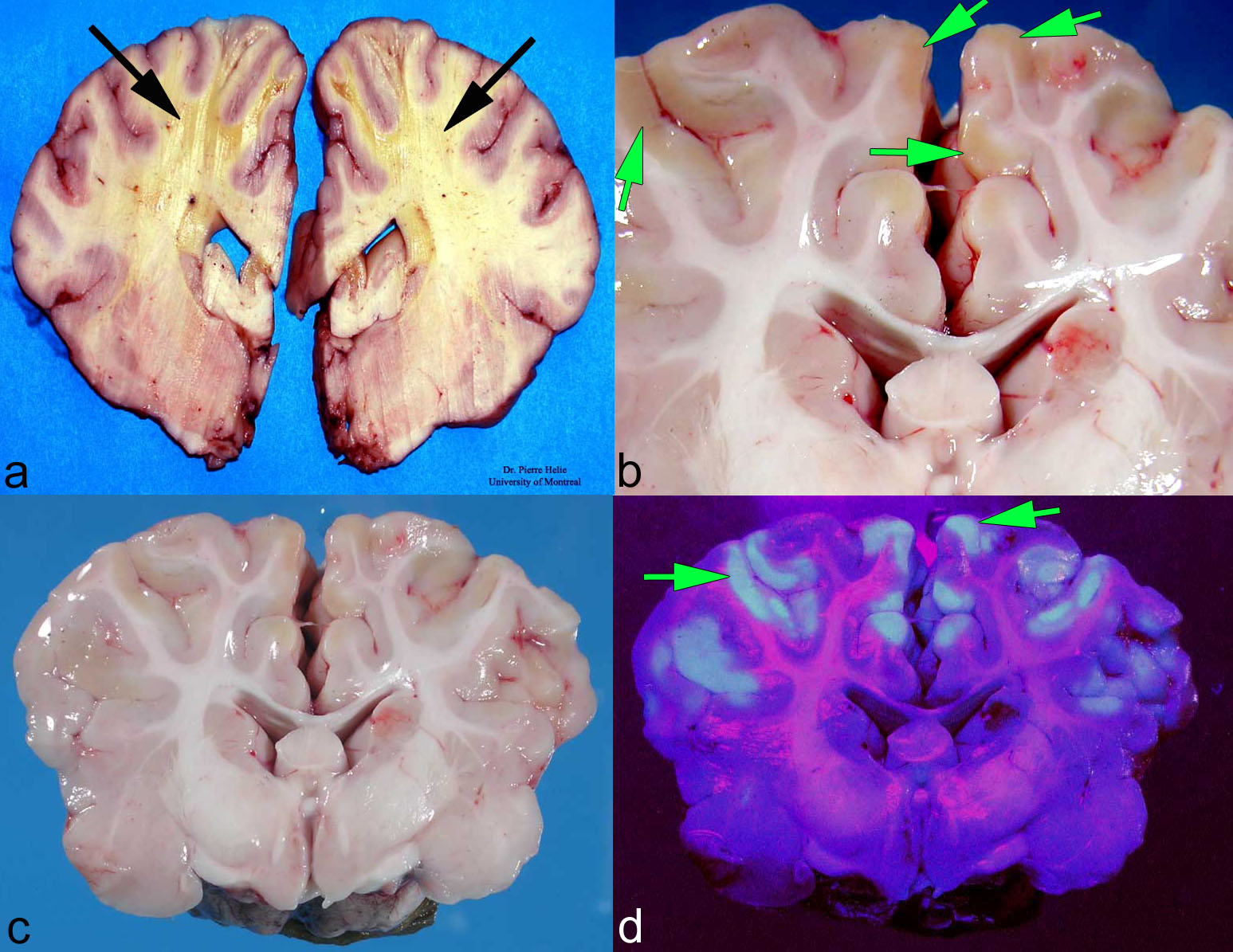
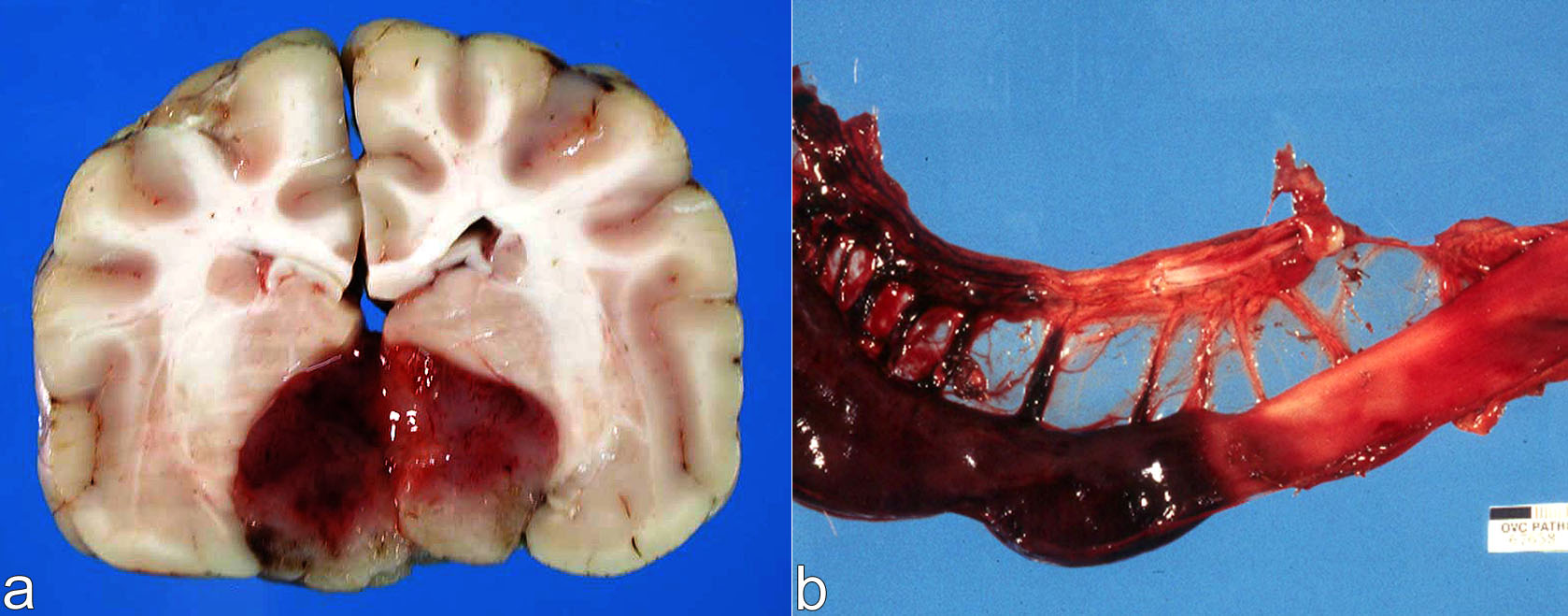
Location points us toward the diagnosis for two cerebral lesions (above and below). (a) Horse. The location of the yellow lesions (arrows, necrosis/malacia) in white matter identifies the lesion as leukoencephalomalacia, caused by ingestion of moldy corn. (b-d) Calf. The yellow lesions (b, arrows; which are auto-fluorescent under UV light in panel ‘d’) are located in the cerebral cortical grey matter. This location identifies the disease as polioencephalomalacia (malacia = softening/necrosis, polio = grey matter, encephalo = brain). The cause in this case was sulfur toxicity, from excessive levels of sulfur in the drinking water.
Dog, sectioned right and left limbs. The location of the dark discoloration specifically involves the distal extremities of all four limbs. This consistent location suggests ischemia as the mechanism of tissue damage, and was probably the result of sepsis in this case. Differential diagnoses could include frostbite, or in calves ergot toxicity that causes vasoconstriction of arteries in distal extremities.
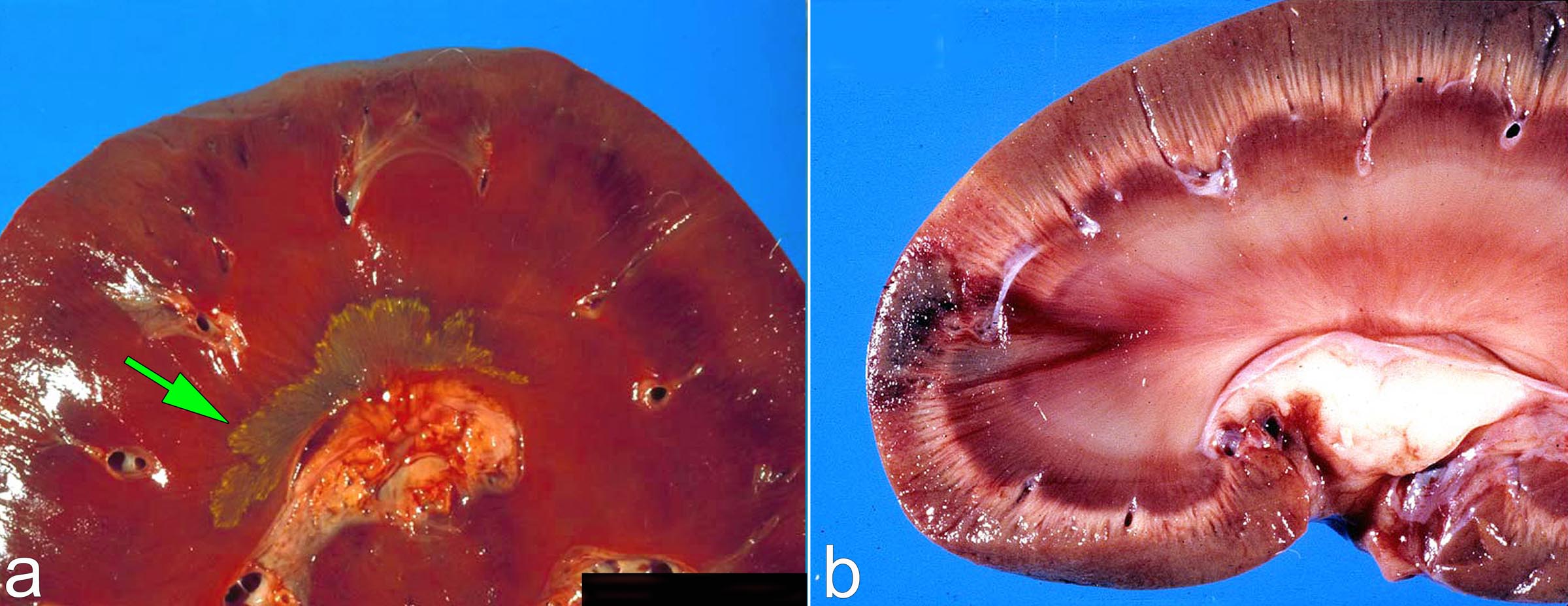
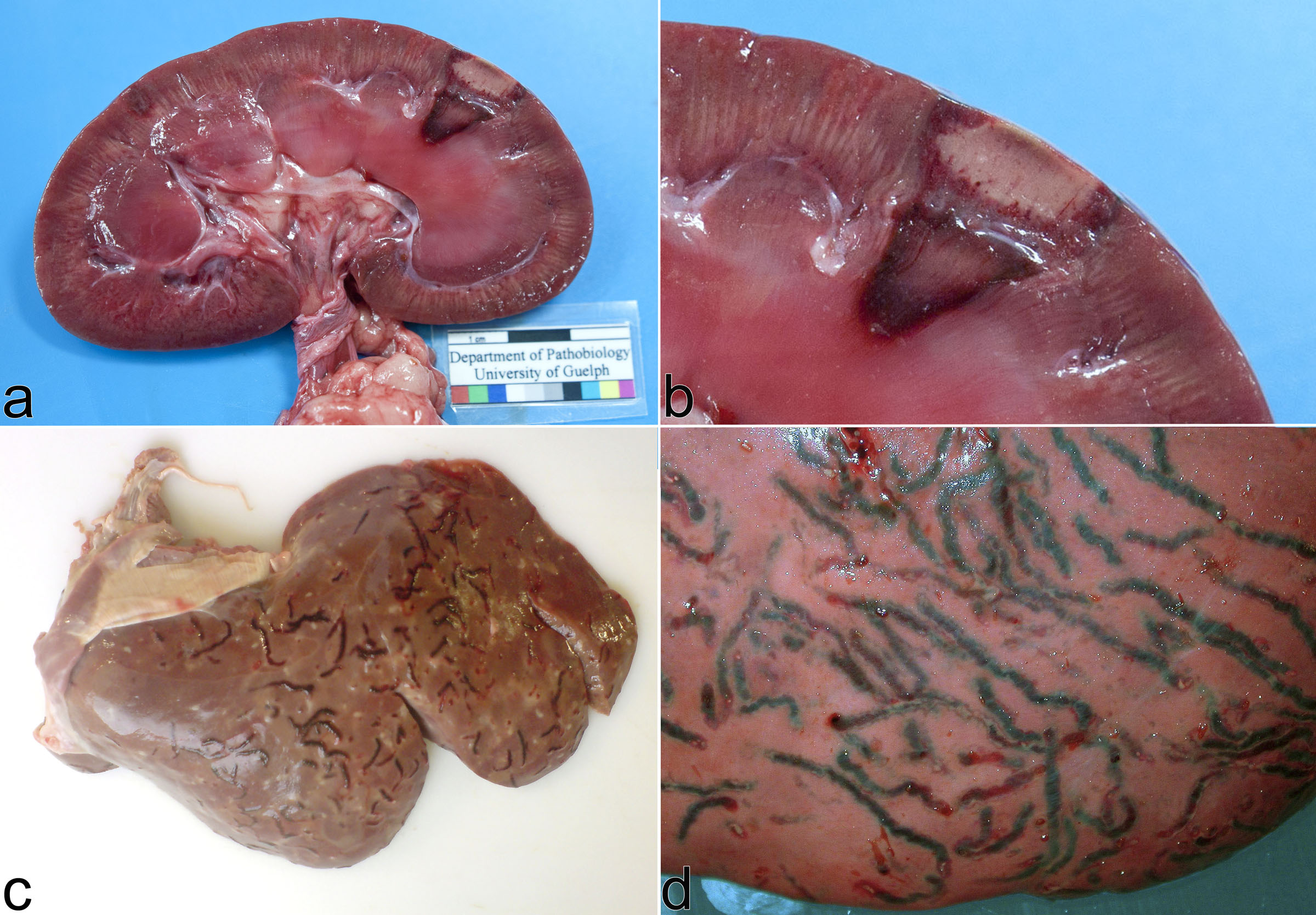
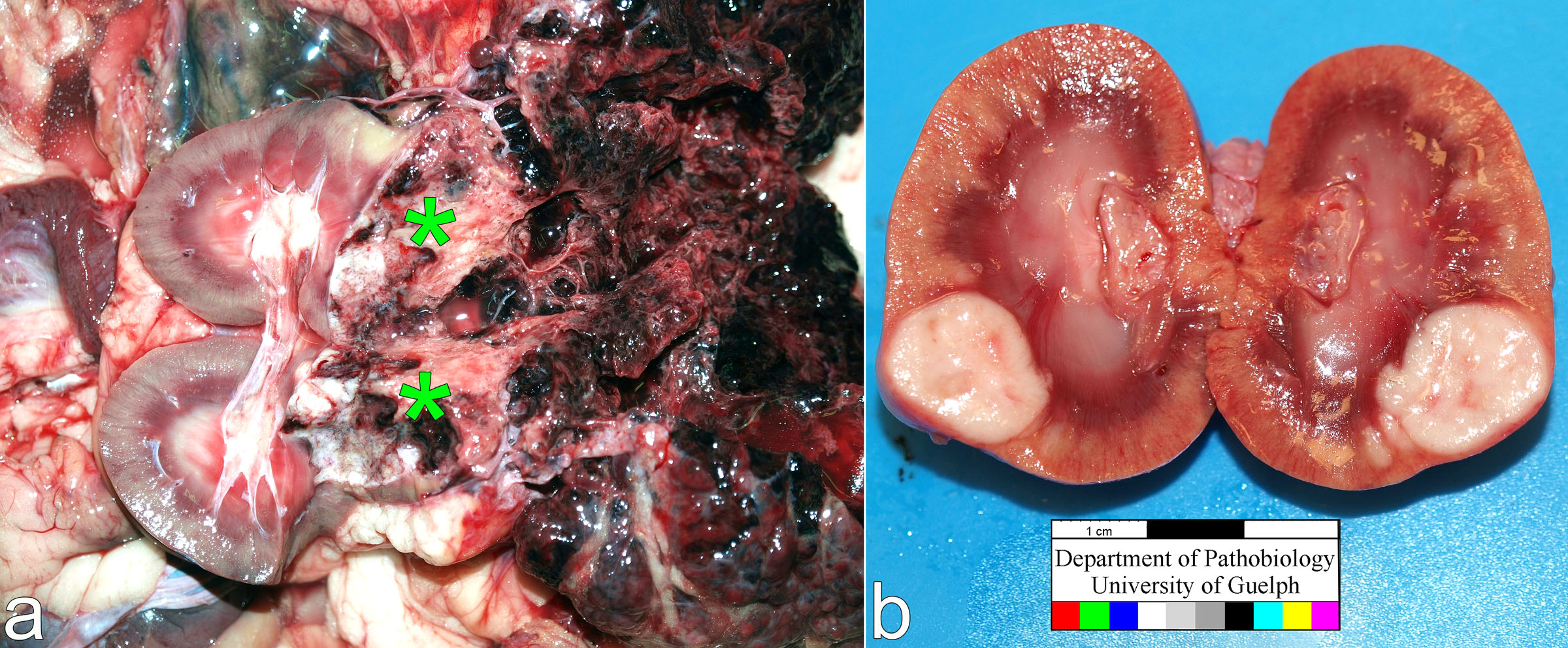
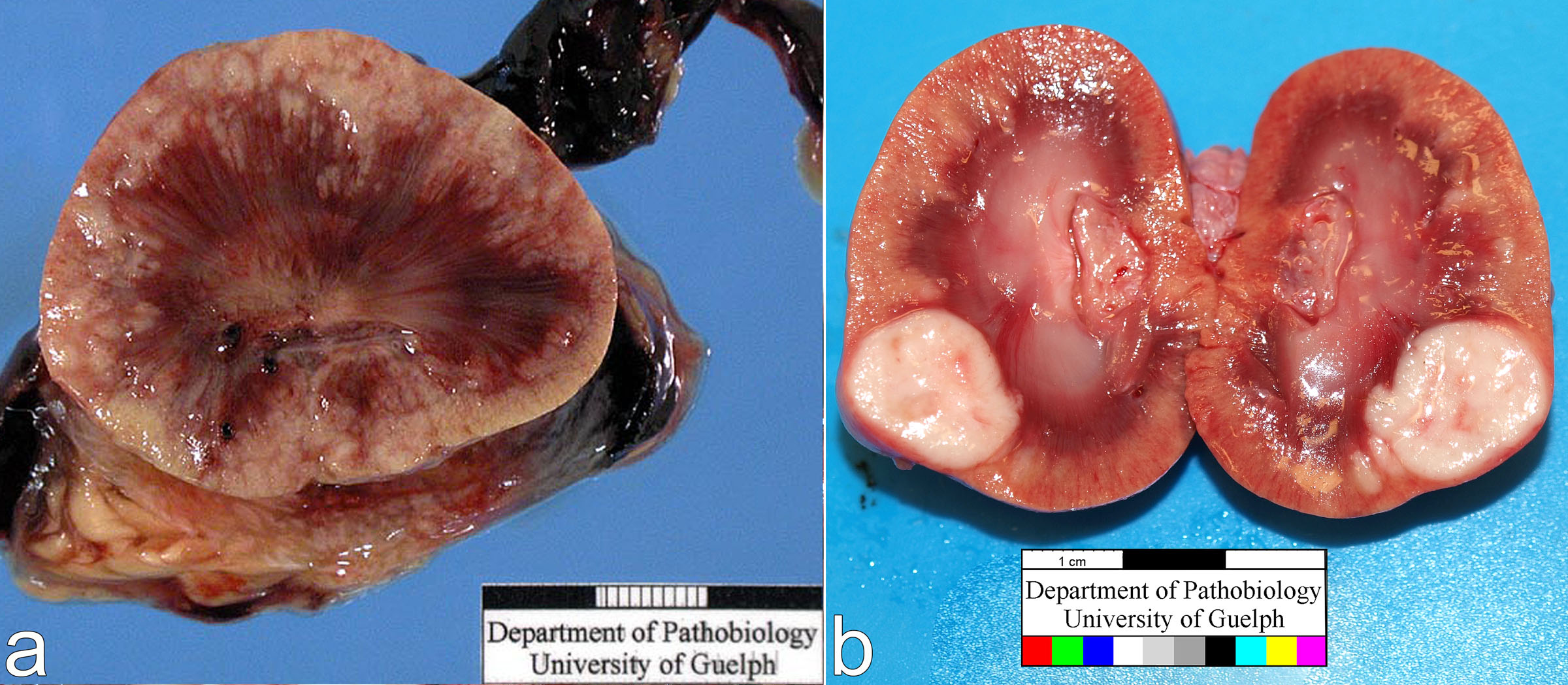
Location of lesions in different parts of the kidney tells us about pathogenesis and cause. (a) Horse. The location of the olive green lesion in the deep medulla is characteristic of ischemic damage due to overdose of nonsteroidal anti-inflammatory drug, given for control of colic. (b) Dog. The cortical location of the triangular lesion identifies it as a renal infarct, due to obstruction of the arcuate artery by a thrombus.
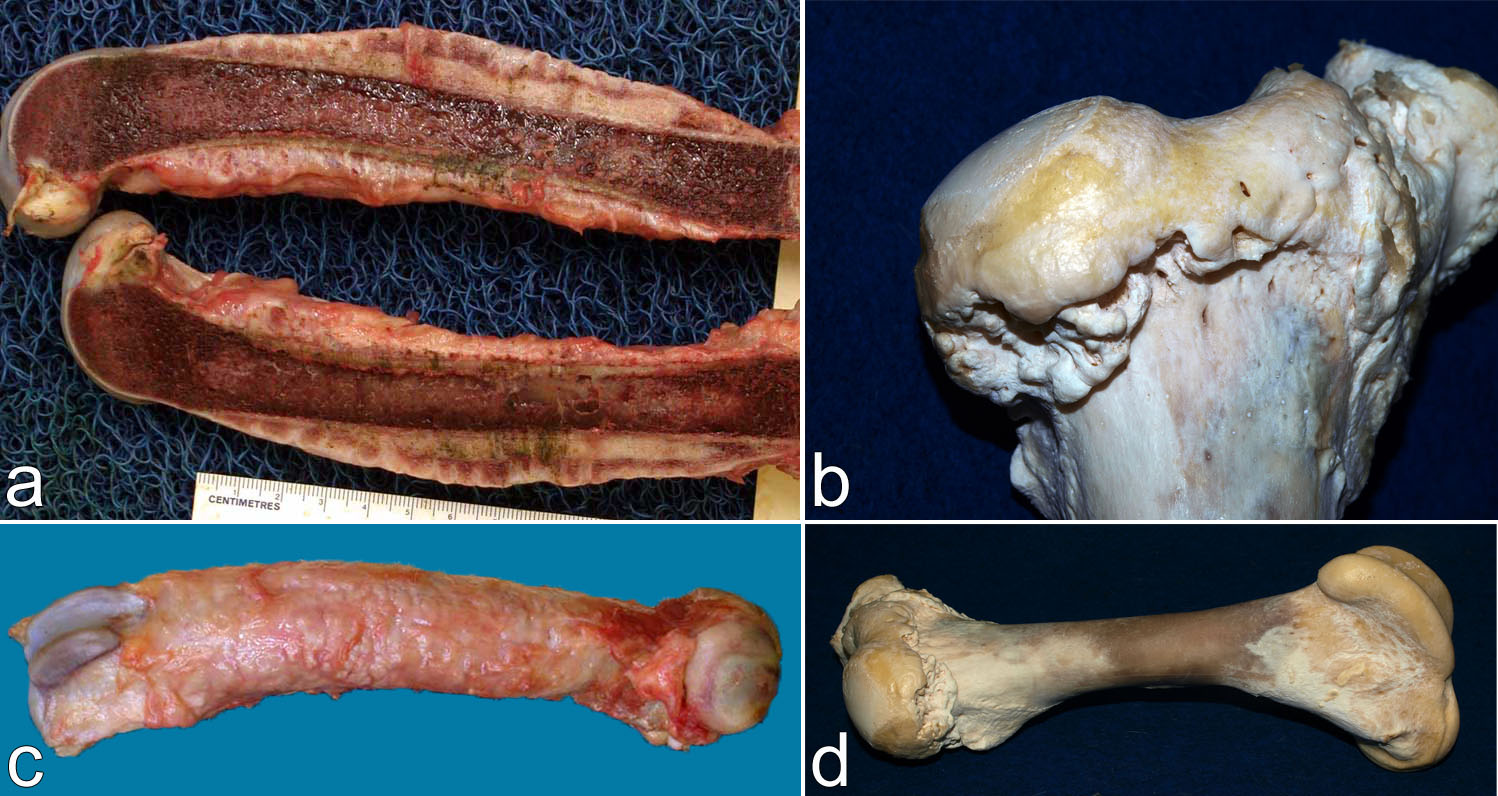
Two lesions of periosteal new bone formation. (a,c) Dog. The lesions affects the entire diaphysis but spares the epiphyses. This lesion distribution is typical of hypertrophic osteopathy. This disease usually develops secondary to a lung mass. (b,d) Cow, new bone formation in the epiphysis adjacent to the joint. This location suggests the bone proliferation is due to chronic arthritis. Erosion of the humeral head from chronic arthritis is also visible in the photo.
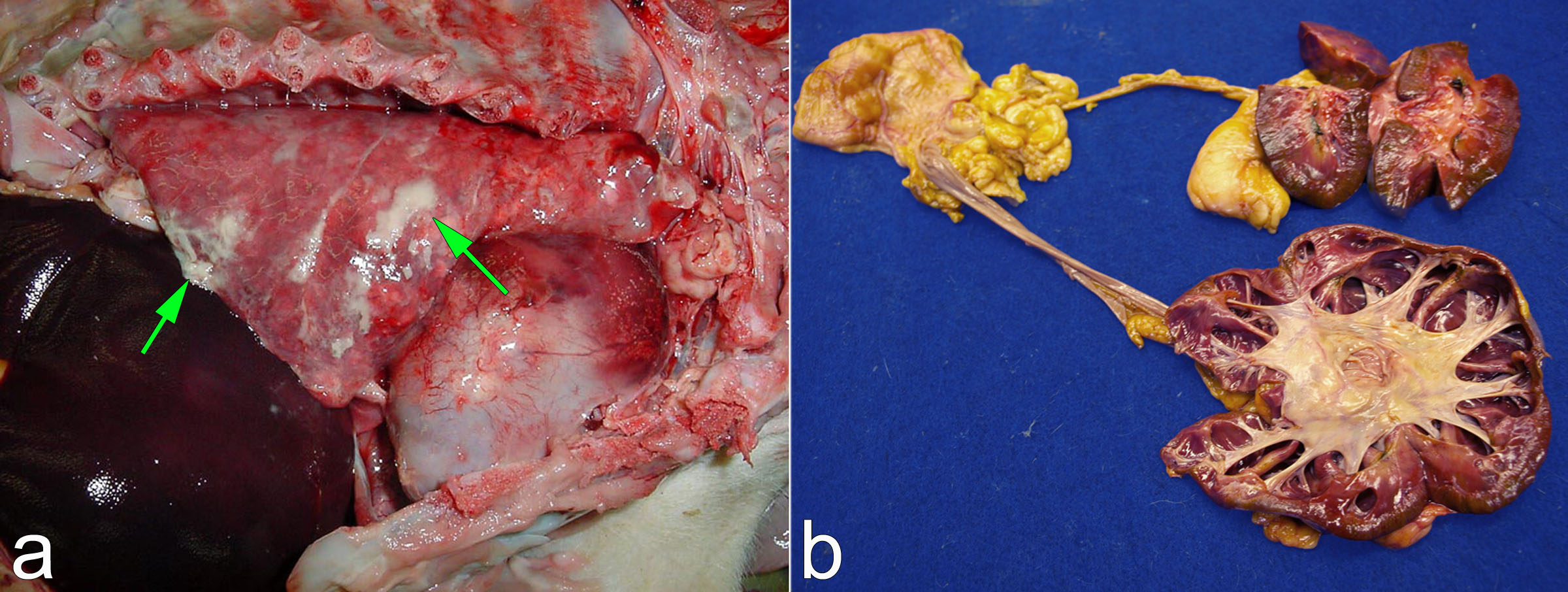
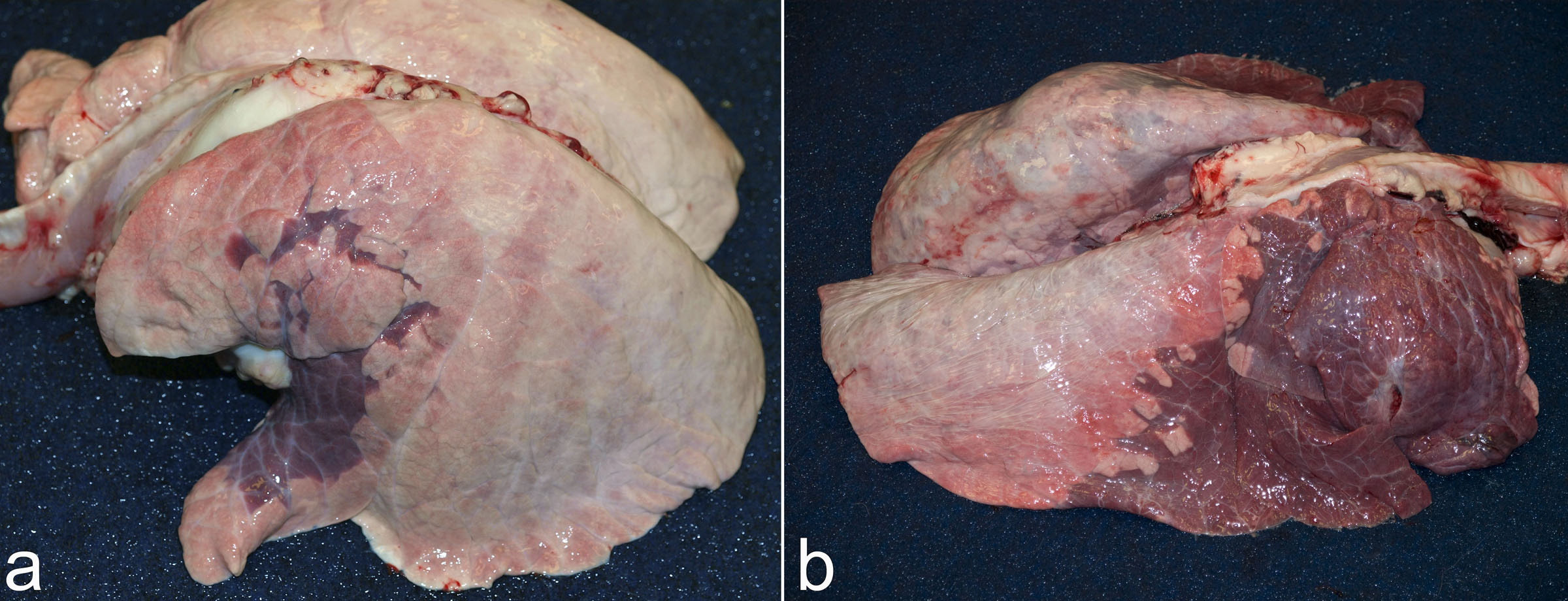
(a) Pig, thoracic cavity. Fibrin is present on the pleural surface (arrows). The lesion does not affect the lung parenchyma (alveoli), but only the pleura. Compared to fibrinous pneumonia, fibrinous pleuritis has different causes, different effects on lung function, and implies a different route of infection. Thus, the precise location of the lesion within the organ (i.e. pleura rather than lung parenchyma) is a key diagnostic feature. (b) Dog. Clue #1: the dilated spaces in the kidney at bottom right are expanded renal pelvis. Clue #2: the lesion affects only one of the kidneys. These features can only be explained by unilateral ureteral obstruction leading to pressure-induced atrophy of renal parenchyma. In this case, the ureteral obstruction was caused by a urothelial (transitional cell) carcinoma.
Distribution: diffuse
Diffuse: the tissue is affected uniformly, like a gas diffusing through the air. The colour on a solidly painted wall has a diffuse distribution. Multifocal or zonal are opposites of diffuse.
Unless otherwise specified, diffuse lesions are assumed to be generalized (present in all areas of the organ or tissue). “Localized diffuse” lesions are usually termed focal or localized.
Extensive patchy lesions may blur the distinction between diffuse and multifocal: diffuse lesions may differ in intensity across a tissue.
Diffuse lesions imply a uniform exposure and response of the tissue to the disease- causing stimulus.
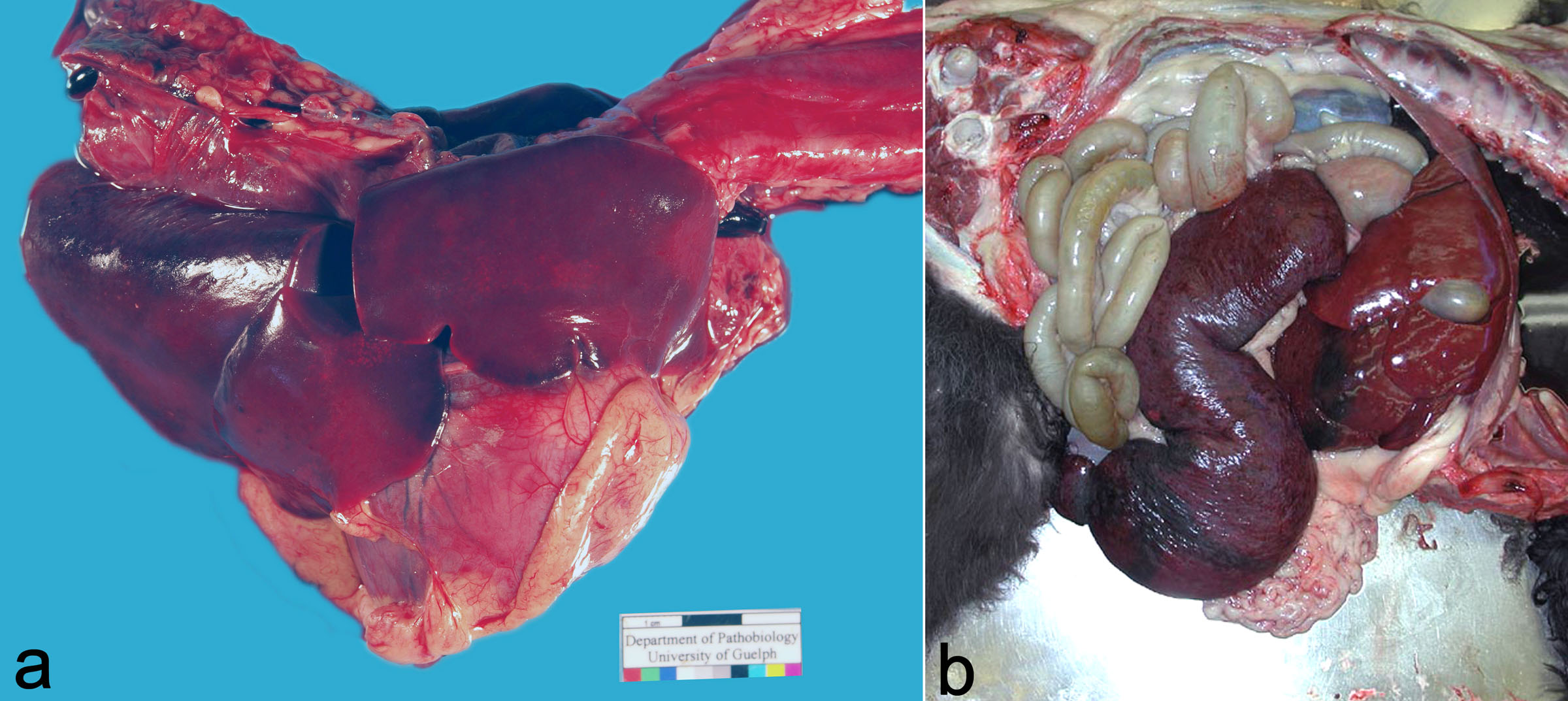
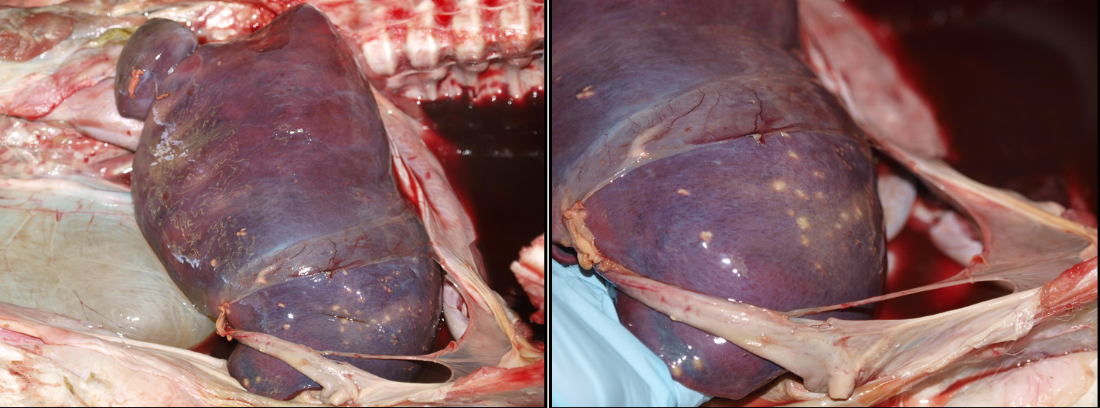
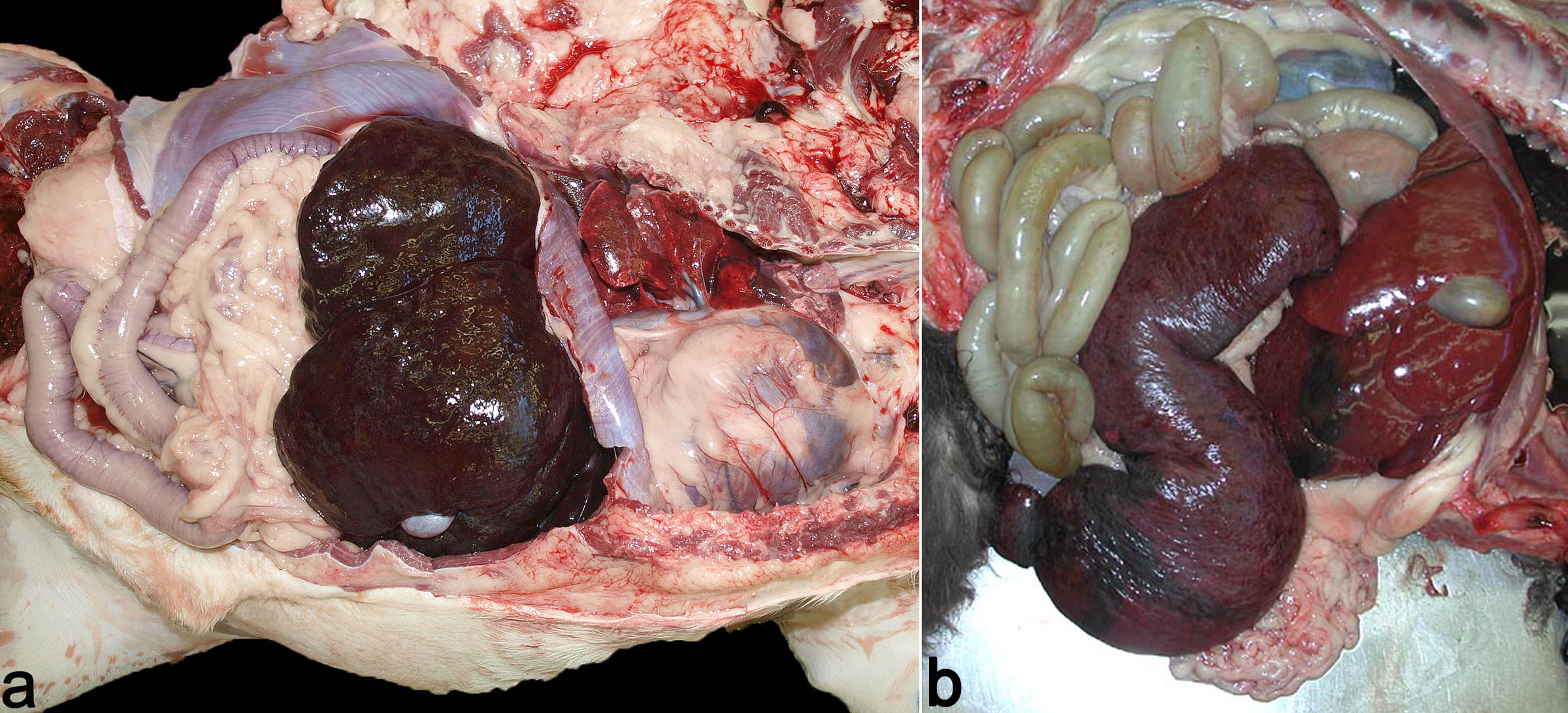
(a) Dog. The lung is diffusely red, and firmer than normal with a liver-like texture. This diffuse distribution indicates a diagnosis of interstitial lung disease, which suggests specific causes. This case was a small dog with neck trauma induced by a bigger dog, and the diffuse lung lesions are thought to result from negative intrapulmonary pressure in an attempt to inspire against the obstructed upper airway. (b) Dog. The spleen is uniformly enlarged. Diffuse splenomegaly was caused by leukemia with blood-borne immigration of neoplastic leukocytes. The diffuse nature of the lesion distinguishes this from other neoplasms such as lymphoma or hemangiosarcoma. Diffuse splenomegaly could also be caused by immune-mediated hemolytic anemia. In that disease, there is hyperplasia of the splenic macrophages that ingest and destroy erythrocytes, as well as new red cell production within the spleen (extramedullary hematopoeisis) to help the bone marrow produce more erythrocytes.
Two dogs with jaundice caused by liver disease. (a) The body is diffusely icteric. This does not mean that all parts of the body are yellow, as the hair remains white, and the muscles and heart are still red. But all parts that are capable of yellow discoloration by bile pigments have turned yellow. This dog had acute liver failure possibly caused by adverse drug reaction. (b) Diffuse jaundice, visible as yellow discoloration of the intima of the aorta. This dog had chronic liver disease of unknown cause.
Cow. Diffuse thickening of small intestinal mucosa that results in a corrugated appearance. This is paratuberculosis (Johne’s disease). The diffuse lesion reflects the widespread distribution of the cause (Mycobacterium avium ssp paratuberculosis) in the small intestinal mucosa.
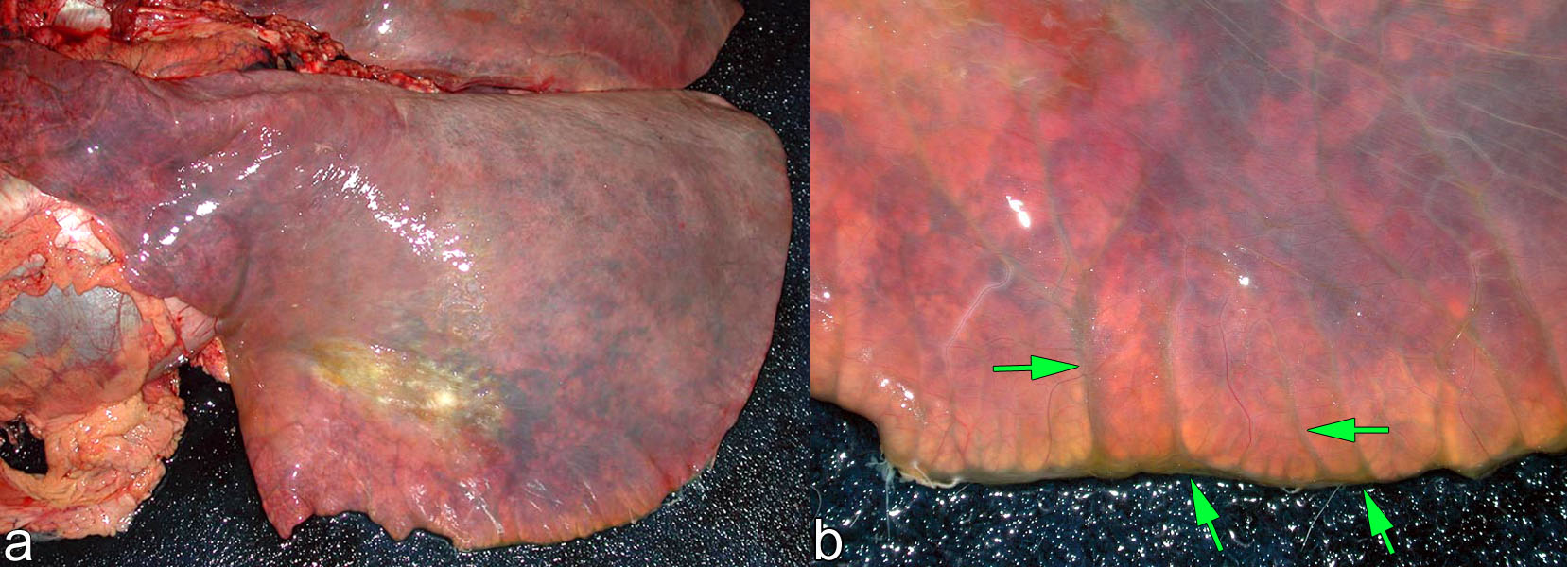
Pig lung. The interlobular septa are diffusely expanded by clear fluid (edema). The lesions affects the interlobular septa uniformly, although the lung tissue itself is not visibly affected. Thus, the lesion is considered diffuse within the interlobular septa.
distribution: generalized random multifocal
Generalized: lesions are present in all parts of the organ or tissue. Generalized is the opposite of localized.
Multifocal lesions are usually randomly distributed: lesions have a haphazard distribution, not based on specific anatomic structures. In contrast, zonal lesions may appear multifocal but have a regular (non-random) distribution.
Multifocal lesions vary in shape and surface contour. Many pathologic processes cause generalized multifocal lesions: inflammation, necrosis, neoplasia, hemorrhage, and mineralization.
This pattern generally implies that the stimulus arrived in the tissue by a blood-borne route.
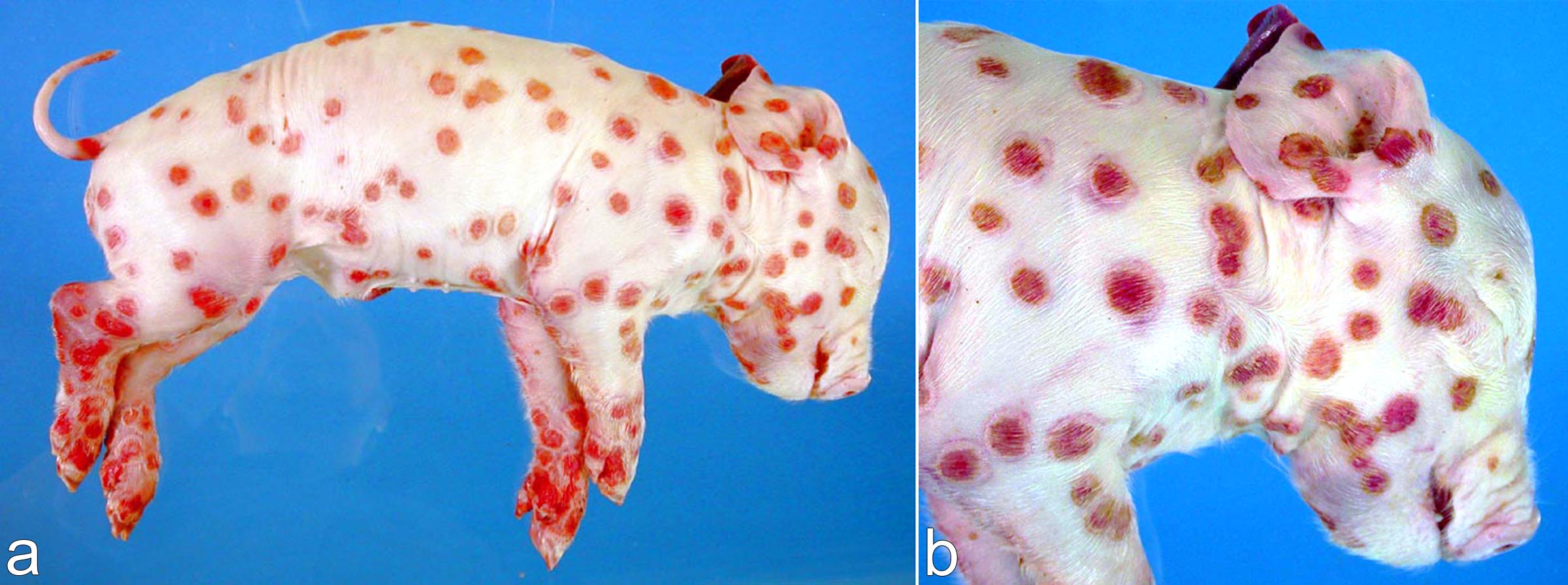
Aborted piglet. The multifocal lesions have a generalized distribution over the entire body surface, and are caused by hematogenous spread of swine pox virus from his mother. The white rims of the lesion represent epidermal hyperplasia (cellular proliferation) induced by the virus, while the red depressed centres are erosions that develop after the infected epithelial cells undergo necrosis. We can learn a lot about pathogenesis by carefully examining gross lesions.
Feedlot steer, esophagus. (a) Esophagus, with larynx at right. (b) Close-up of the esophageal mucosa. Tiny multifocal erosions on the mucosal surface represent necrosis caused by hematogenous spread of bovine viral diarrhea virus. Each focal lesion is a tiny site of viral replication and destruction.
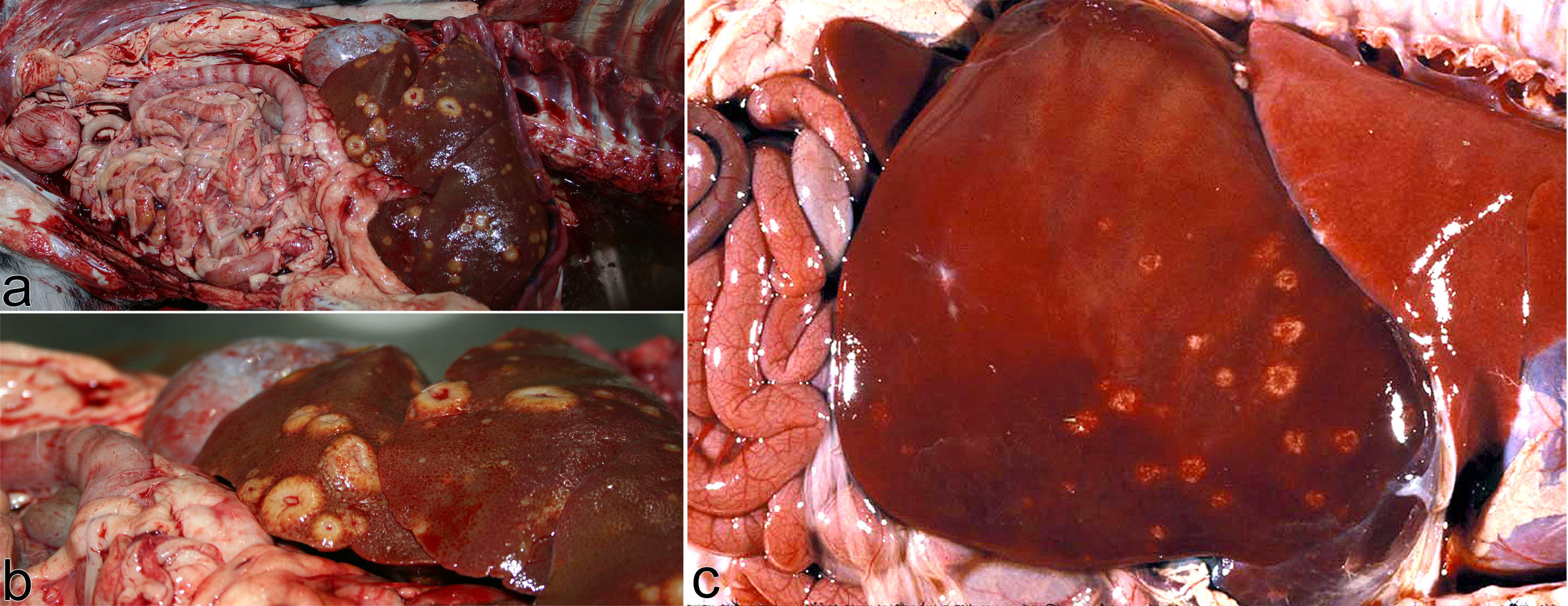
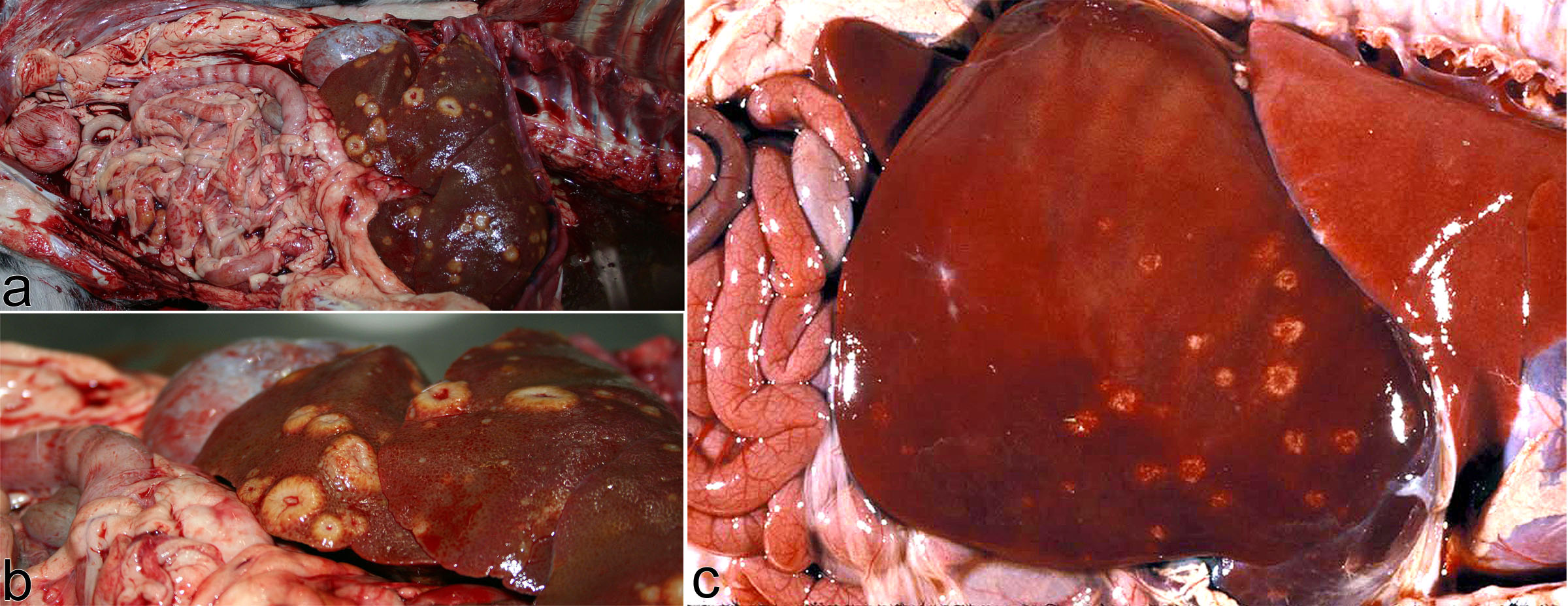
(a,b) Dog. The nodules have a generalized multifocal distribution throughout the liver. This is a carcinoma (malignant epithelial neoplasm) that metastasized to the liver through the blood. The nodules are “umbilicated” (raised, with depressed centres); this appearance results from a scirrhous or desmoplastic reaction (fibroplasia) induced by the neoplastic cells, and specifically by contraction of the fibrous tissue to form these depressions in the centre. (c) Aborted lamb. Multifocal raised “target- shaped” lesions in the liver, representing inflammation and necrosis caused by hematogenous spread of Campylobacter fetus subspecies fetus. This target-shape of the lesions is characteristic of this disease. So, these two cases also provide an example of how precise observation of gross morphology suggests a more specific diagnosis (a: carcinoma rather than just neoplasm, and b: Campylobacter rather than just “infection”).
distribution: focal
Focal: a single lesion, that may be well- or poorly-demarcated. This pattern implies a single point exposure to a damaging stimulus (eg. focal trauma), a rare event occurring once (eg. development of a benign neoplasm), or a lesion filling a single anatomic structure.
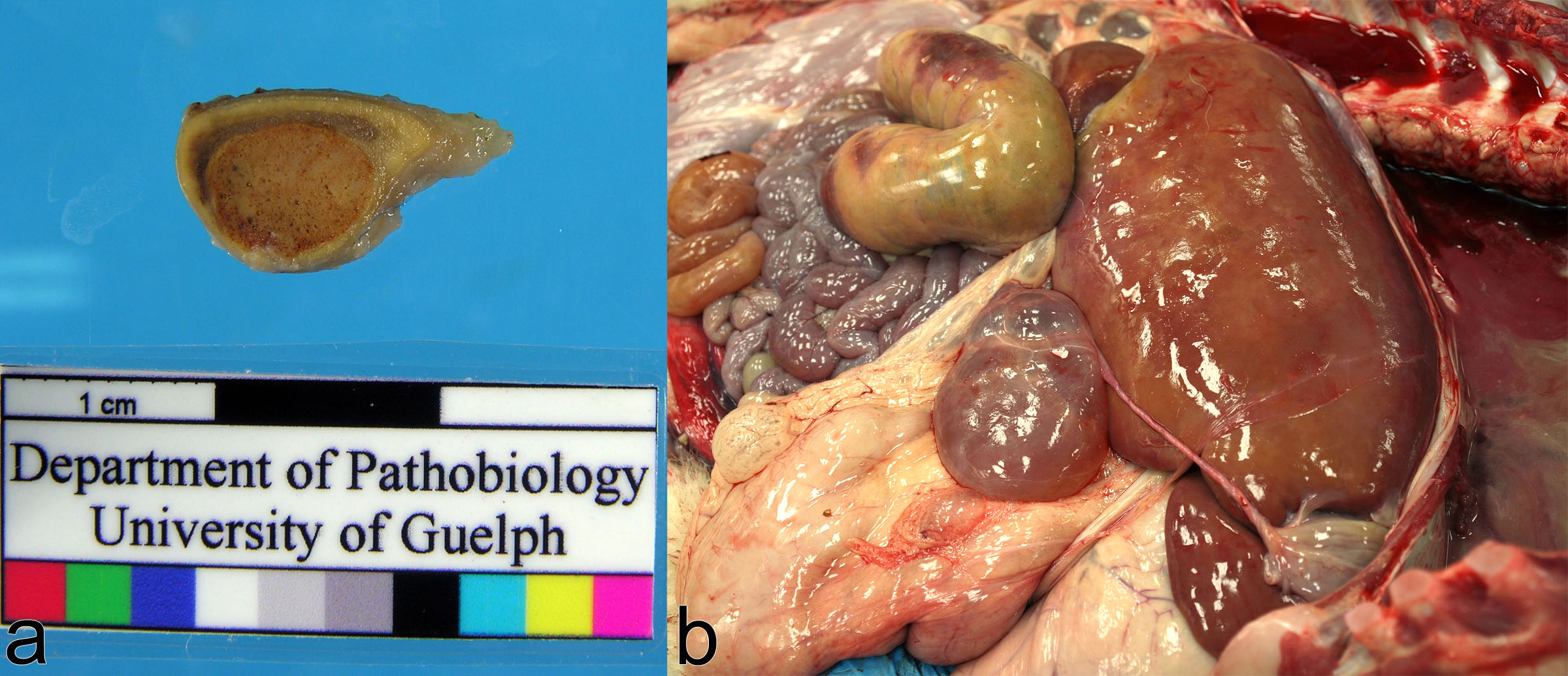
(a) Dog, adrenal gland. A focal adrenocortical adenoma expands the cortex. Neoplastic transformation is a rare event, and the single mass arises from this clone of transformed cells. (b) Dairy calf. A focal cystic lesion arises from the liver. This is a cyst of biliary origin and is though to be incorrect development of the bile duct within this focal area of the tissue. It’s just a single lesion affecting a small amount of liver, and it is not expected to affect organ function or the health of the calf. This lesion could also be considered as localized rather than focal.
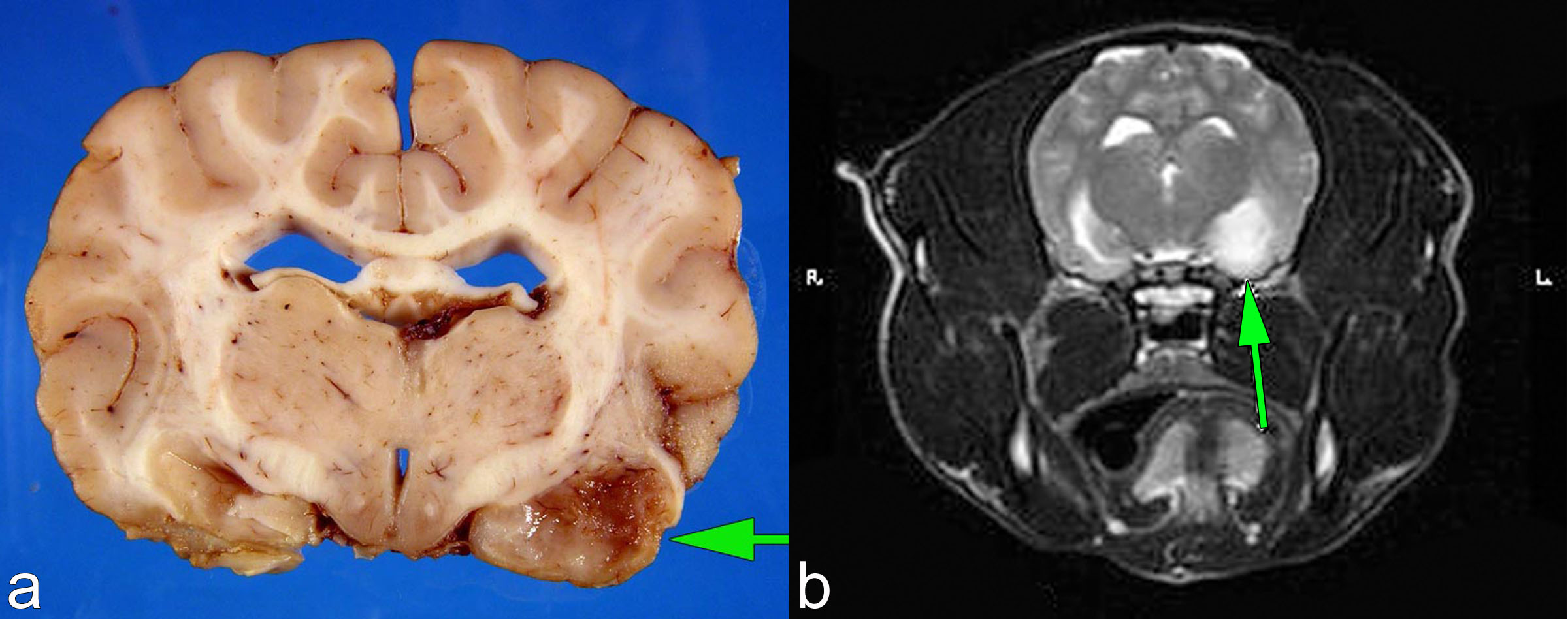
Dog, brain. A focal neoplasm in the pyriform lobe (arrow). The diagnosis was malignant astrocytoma. Neoplastic transformation is a rare event, so there is only one focal lesion. But in contrast to the calf above, the location of the lesion in this case is unfortunate because it induced seizures that eventually resulted in death. In the calf’s liver, the cysts only compromise liver function by a “space occupying” effect, and >60-75% of the liver has to be affected before it causes liver failure. But for the dog’s brain tumour, a small proportion of the brain is affected but it caused death because it impinged on vital structures in this area of brain. So, the functional importance of a focal lesion depends on its anatomic location, and its growth habit.
Distribution: localized
Localized: involving one part or area of a tissue: the opposite of generalized.
Single small lesions are usually termed focal. In contrast, the term localized is used to describe larger lesions that don’t affect the entire tissue. A splash of wine on a white carpet makes a focal lesion; a spilled pail or a cracked water pipe floods a localized area of the basement.
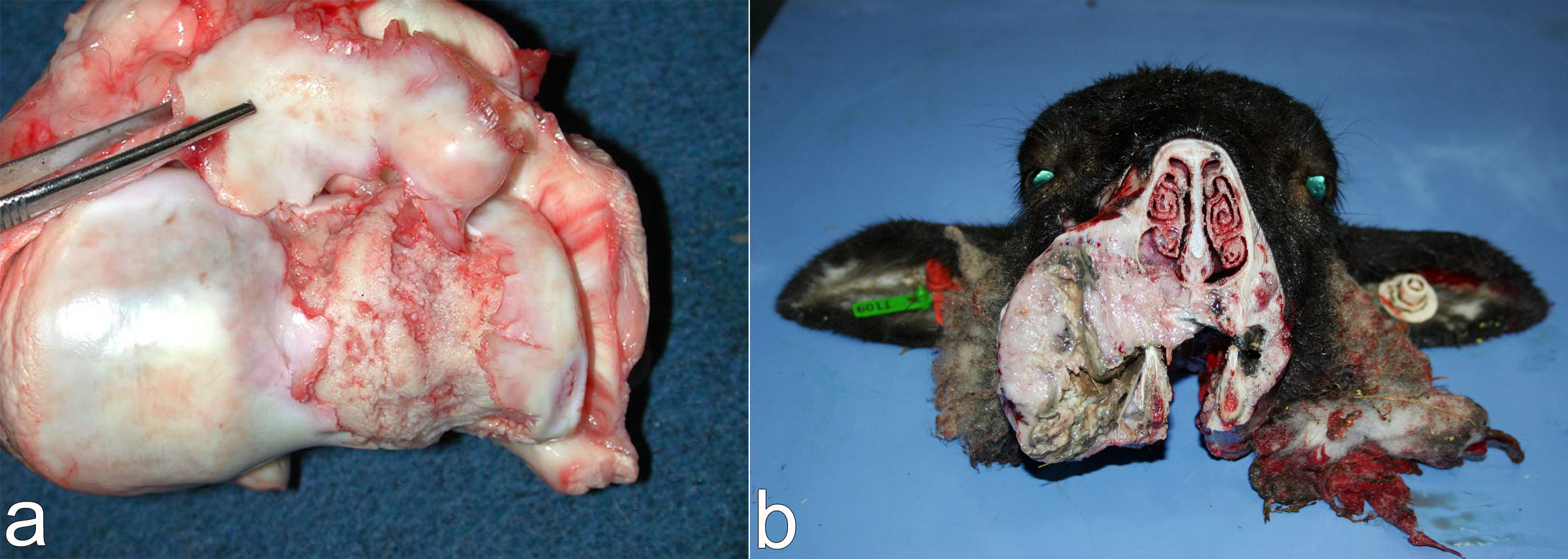
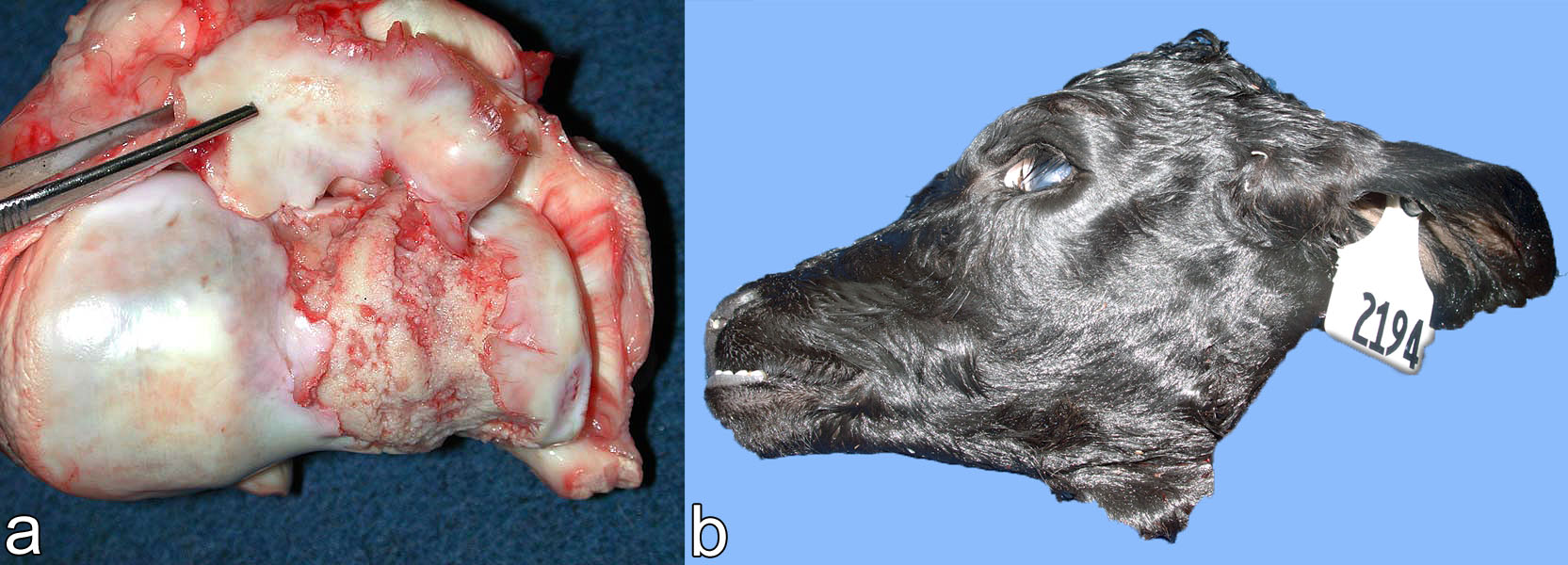
(a) Horse. Osteochondritis dissecans, causing localized detachment of the cartilage. The localized nature of the lesion reflects either abnormal trauma on this area of the cartilage, and/or localized disruption of vascular supply to this area of cartilage as the cartilage developed earlier in life. (b) Sheep. Localized osteomyelitis of maxilla, due to bacterial infection penetrating from the oral cavity. The chronic inflammation incites new bone formation in the area of the infection. The localized nature of the new bone formation reflects the spread of infection from the oral cavity into a localized area of bone.
Neonatal calf, liver. Showering of bacteria from the umbilicus caused a localized area of multifocal suppurative inflammation. The lesions are localized rather than generalized, because the umbilical vein selectively perfuse the right side (not the left side) of the liver. A reminder the umbilical vein delivers blood from the placenta to the calf, and it runs from the umbilicus into the liver (then in a fetus, blood travels via the ductus venosus into the caudal vena cava). So, this is a cool example of a multifocal distribution that is localized rather than generalized.
Horse. Bacterial infection of the right hind limb has induced inflammation, resulting in edema of the affected area. The edema is not generalized throughout the body, but instead is localized to the area of the infection.
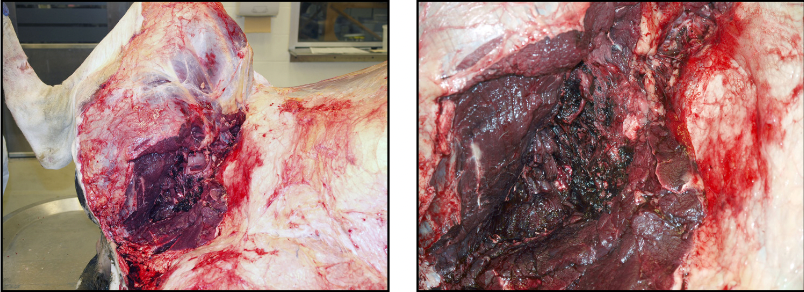
Cow. Hemorrhage in the soft tissues, due to luxation of the hip joint. The left photo shows the medial aspect of the hindlimb including the dislocated hip joint. Either focal or localized is appropriate to describe the distribution of this lesion. It is localized to the area that suffered the trauma.
distributions corresponding to specific anatomic structures
Identifying the anatomic basis for the location or distribution of a lesion provides an important clue to understanding how a lesion developed.
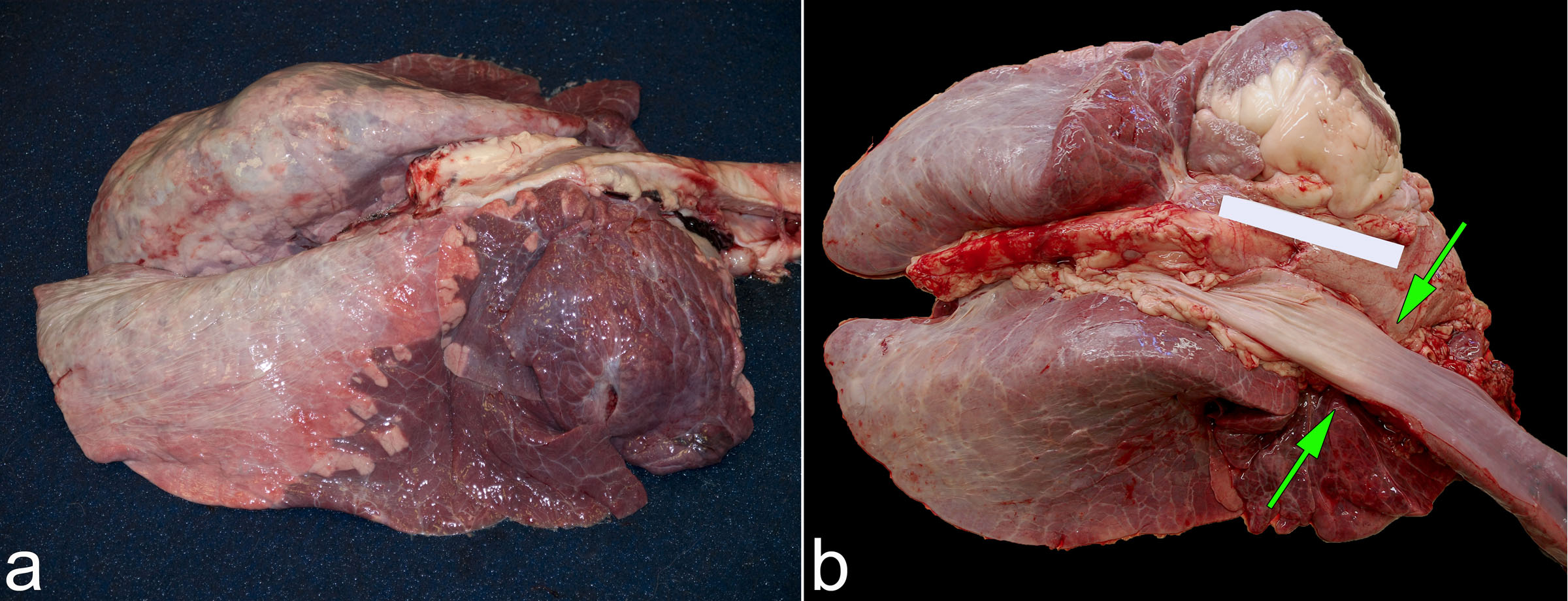
Dog, thoracic cavity. The right middle lung lobe has undergone venous infarction as a result of torsion. The site of torsion is visible in photo “b”. The fact that the lesion affects one entire lobe (i.e. lobar) suggests torsion as one possible cause.
(a) Dairy calf, lung. These cranioventral lesions of bronchopneumonia have a lobular distribution. At the junction of normal and abnormal, it is apparent that some lobules are entirely affected (purple-tan) while others are normal (salmon pink). This tells us there has been a slow spread of infection via the airways, with enough time to involve some lobules entirely but spare others. (b) Calf, pluck. The cranial part of the esophagus is red due to congestion, while the caudal part is blanched due to exclusion of the blood. This is a “bloat line”. In bloated calves, distention of the rumen forces blood from the abdominal and thoracic cavities and obstructs venous drainage from the head and neck, leading to the changes observed. The key observation is that the line of demarcation (the “bloat line”) corresponds to a specific anatomic structure, the thoracic inlet.
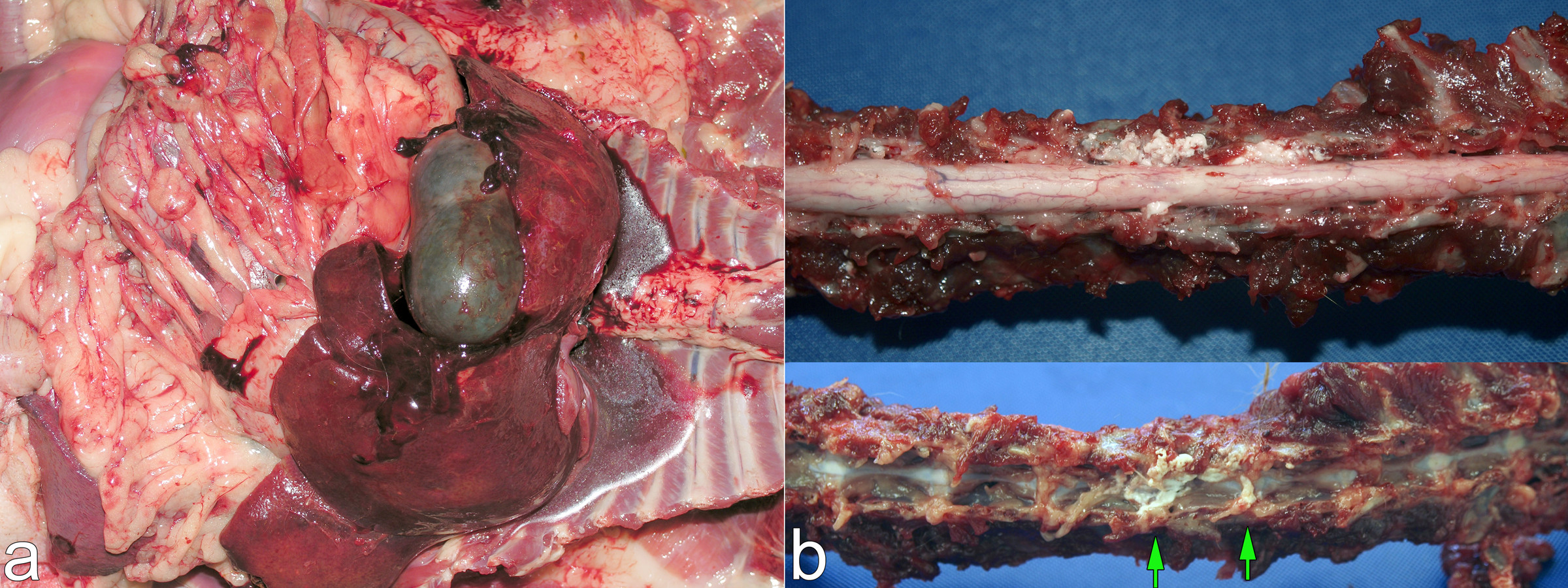
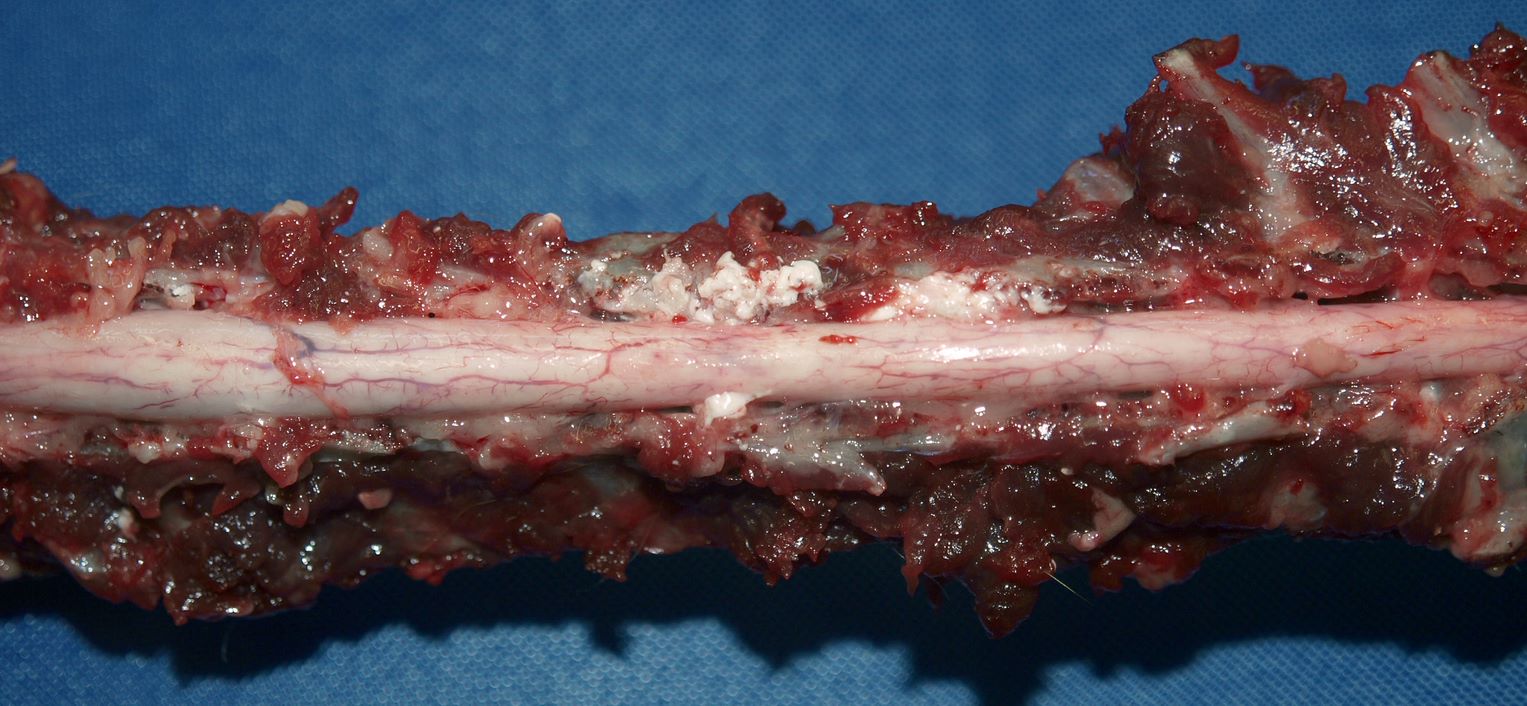
(a) The green mass is focal and well-demarcated because it is a single anatomic structure, the gall bladder. Dog, gall bladder mucocele. (b) Dog, spinal column with dorsal laminectomy revealing the spinal cord (top), and with the spinal cord removed (bottom). Recognizing the white friable material (arrows) as extruded disk material is easy, once it is identified that the location corresponds to the intervertebral disks.
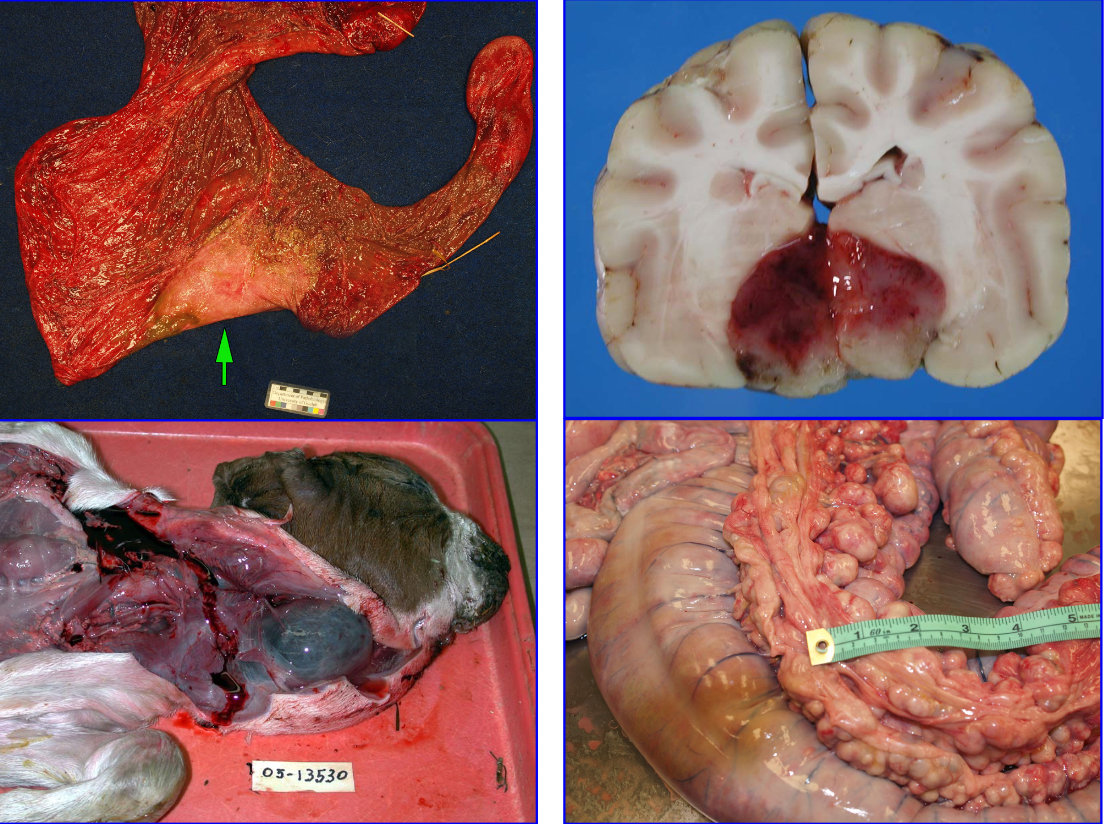
The diagnosis in each of these cases requires identification of the specific anatomic structure affected by the lesion: Top left: Mare, Nocardia placentitis. The pale area of necrosis and inflammation affects the area adjacent to cervix, suggesting that the pathogen entered the uterus via the cervix and vagina. Top right: Dog, pituitary adenoma. The location of the tumour corresponds to the pituitary gland, with expansion into the hypothalamus. Bottom left: Aborted goat kid. Bilateral masses in the expected location of the thyroid glands. Identifying the masses as thryoid gland leads to the diagnosis of , goitre due to iodine deficiency. Bottom right: Foal, colonic lymphadenitis caused by Rhodococcus equi. Recognizing the mesocolonic masses as lymph nodes is key to the diagnosis.
Caribou, distal limb. The pus-filled tracts correspond to the joints and tendon sheaths, and this explains the distribution of the lesion in the distal limb. There was excessive stubble this year, which were thought to have caused penetrating damage to the foot, inoculating bacteria into the joints and tendon sheaths.
size & Extent
Size and extent of lesions could be given as the absolute dimensions (for example, in centimeters), or as the weight of the affected organ or lesion, or as the percentage of the tissue that is affected by the lesion. Each of these measurements provides information of different value, which will be more or less useful depending on the context.
Above: These two lesions are nearly identical except for the percentage of lung tissue affected. In organs where the tissue mass is relevant to function (such as lung, liver, kidney, intestine, and endocrine glands), it is essential to state the percentage of tissue affected.
Horse, post-surgical pulmonary edema. (a) Edema is difficult to appreciate in the photo. (b) Edema fluid is present in interlobular septa and at the apices of the lung (arrows). In this case, describing the weight of the affected tissue compared to normal would be an objective way to communicate the magnitude of the edema. These lungs are much heavier than normal because they are partially filled with water (edema).
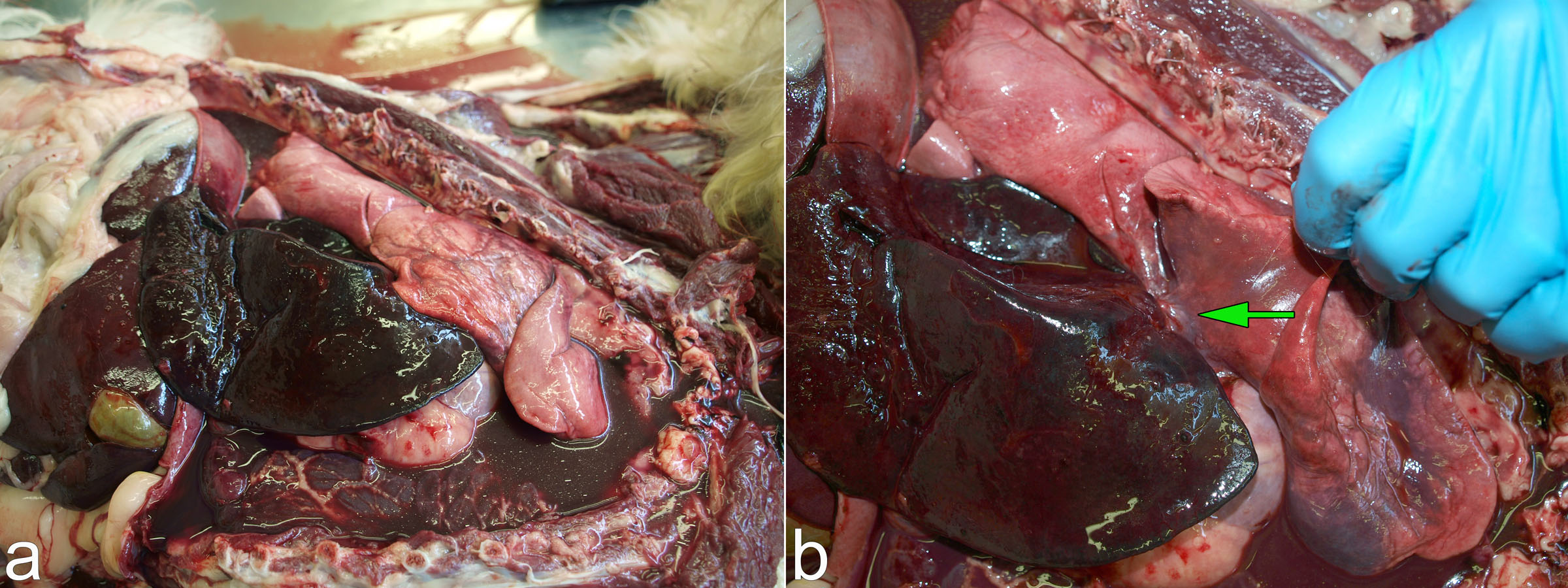
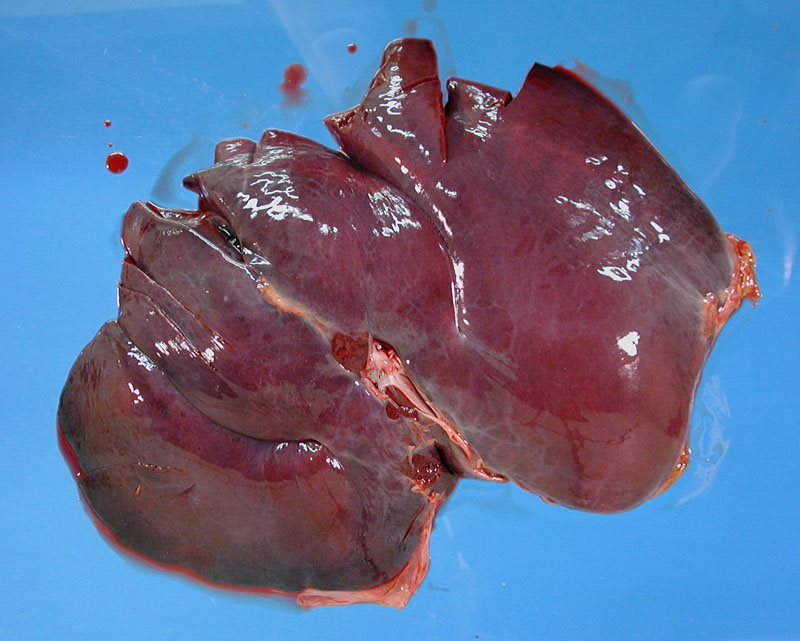
(a) Dog, enlarged and congested liver due to right heart failure. Note the globose heart. The size of the liver could be effectively communicated by stating that it is about 50% larger than the normal liver in image “b”, or by stating its mass of the liver (in grams) compared to a normal range for dog liver. (b) Dog, splenomegaly due to leukemia. This could similarly be communicated by stating the size relative to normal, or the weight in relation to a normal range.
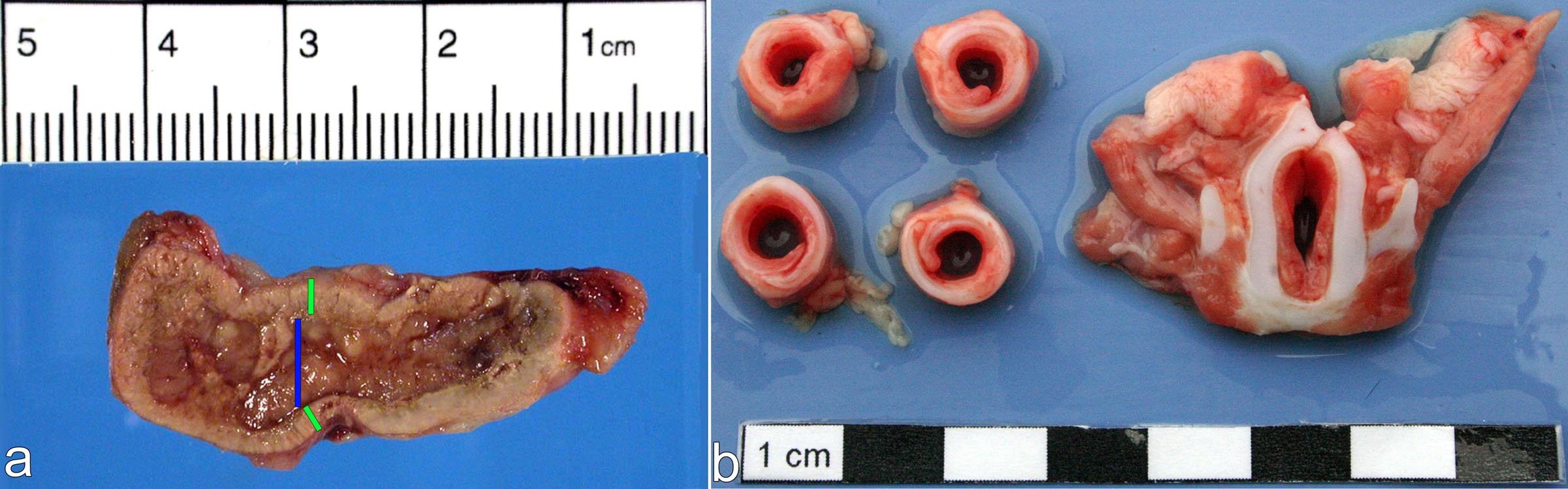
(a) Dog, atrophy of adrenal cortex causing hypoadrenocorticism. The size of the adrenal cortex could be described as 2-3 mm thick, but interpreting this information would require knowledge of the size of the dog, and the thickness of the cortex in dogs of various sizes. The thickness of the adrenal cortex is more often described as a ratio of cortex to medulla. In the photo, the green and blue lines show the thickness of the cortex and medulla, respectively. The cortex: medulla in normal animals is about 1:1, but it is 1:3 in this case. There has been destruction of the adrenal cortex so it is now much thinner than the medulla. The atrophied cortex makes less hormone, leading to the clinical syndrome of hypoadrenocorticism. (b) Bulldog, brachcephalic obstructive airway syndrome. In this case, the reduced diameter of the tracheal and laryngeal lumen could be expressed as an absolute size, or as an estimated percentage of normal. For example: The laryngeal lumen is narrowed to 5 mm with 2-fold thickening of the mucosa. The trachea has outer and inner diameters of 5 and 10 mm respectively, with overlapping of the ends of the tracheal cartilage. This observation of overlapping ends of the cartilage is interpreted as collapse due to excessively negative intratracheal pressures during inspiration. Note that these findings represent the dimensions in death, but muscular contraction may have held these structures open in life. Photo credit: Brian Cloak, Univ. Coll. Dublin.
Shape
(a,b) Dog, liver, cholangiolar (biliary) adenocarcinoma. Umbilicate lesions—nodules with depressed centres like an umbilicus—are characteristic of carcinomas because the neoplastic epithelial cells secrete growth factors that stimulate desmoplasia, leading to contraction of this fibrous tissue. (c) Aborted lamb, Campylobacter fetus ssp. fetus infection. Target lesions usually represent 2 distinct pathologic processes: in this case, a collapsed red centre of necrosis, and a white rim of leukocyte infiltration as a result of this blood-borne bacterial infection.
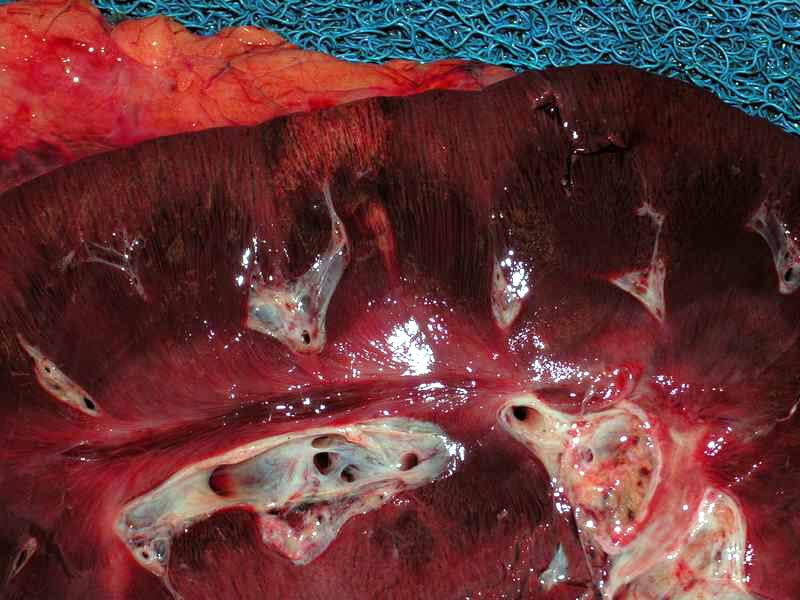
(a,b) Dog, kidney. Triangular lesions usually have a vascular basis: this renal infarct resulted from thrombosis of an arcuate artery, and subsequent ischemic damage. (c,d) Lamb, liver. Serpiginous (snake-like) lesions could be inflammation following the course of vessels, but these wandering tracks in the liver of a lamb are necrosis and hemorrhage due to migration of larval cestodes: Cysticercus tenuicollis. Image credit: Ab Rehmtulla.
Demarcation
A lesion may be well demarcated because:
it grows by expansion, instead of by invasion or infiltration (eg., a benign neoplasm)
it is contained within a capsule (eg., abscess) or an anatomic structure (eg., in a lung lobule, or in the gall bladder)
of the manner in which it arises (eg., the intestinal venous infarct shown below).
(a) Dog, pituitary macroadenoma with growth into the hypothalamus. The mass is well-demarcated because it grows by blunt expansion, and nudges adjacent brain tissue out of the way to accommodate its growth. (b) Horse, small intestinal venous infarction due to a strangulating lipoma, horse. The well-demarcated lesion reflects focal obstruction of the venous drainage by the stalk of the mesenteric lipoma.
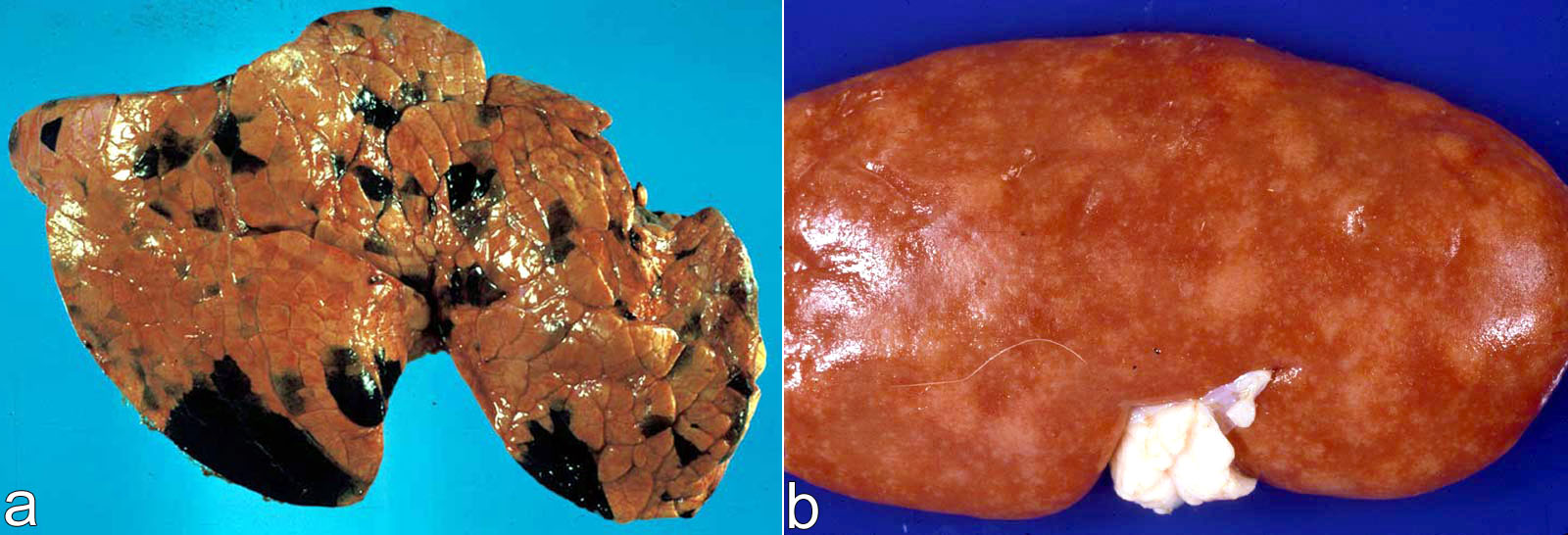
(a) Bovine lung, melanosis. The black lesions are well-demarcated because some lung lobules are pigmented and others are not. In melanosis, the cause of melanin production in these lobules is unknown, but does not affect lung function. (b) Poorly demarcated white foci represent expanding areas of inflammation. Pig, kidney, Leptospira pomona.
(a) Dog, renal adenocarcinoma with invasion (asterisks) and destruction of the kidney and adjacent tissue. (b) Cat, kidney. These well-demarcated tan nodules are metastases to the kidney from a distant primary tumor. Thus, poor demarcation with invasive growth is an indicator of malignancy, but not all malignant neoplasms have invasive growth (metastasis is another indicator of malignant behaviour).
surface contour: depression
A depressed surface contour results from loss of tissue, shrinkage due to atrophy, or contraction of maturing fibrous tissue.
(a) Horse, arthritis caused by osteochondrosis dissecans. The sunken contour of the joint surface from loss of cartilage tissue. The forceps are holding the partially detached flap of cartilage. (b) Sunken eyes in a dehydrated neonatal calf with diarrhea. Because of severe dehydration, the retro-orbital tissue has less tissue fluid than normal, leading to retraction of the eyes.
(a) Dog, kidney. The capsular surface has innumerable, widely distributed, poorly demarcated, 1-3-mm-diameter, tan areas that are sunken compared to the more normal pink tissue. The depressed lesions are areas of interstitial fibrosis and atrophy of renal tubules, resulting from chronic renal disease. (b) Dog, renal infarct (ischemic necrosis due to obstruction of an arcuate artery). Necrotic tissue is usually flat, as in this case, but may be subtly raised due to cell swelling, or subtly depressed due to loss of cells or tissue. The slightly raised lesions caused by acute necrosis are usually much more subtle than raised lesions caused by neoplasia, hyperplasia, or inflammation; and the slight depression caused by necrosis is often more subtle than would occur with fibrosis.
Dog, acute hepatic necrosis, thought to be caused by an adverse drug reaction. (a) The liver is much smaller than normal and has a variegated appearance. (b) A regularly alternating “zonal” pattern of tan-orange and purple-brown areas. It can be difficult to know which of these is normal and which is diseased. The small size of the liver might suggest that the collapsed areas are abnormal. Indeed, in this case, the sunken purple-brown areas were identified histologically as necrosis (and hemorrhage), while the orange-tan areas were the surviving hepatic tissue. The purple-brown areas are depressed because of loss of hepatocytes. This loss of hepatocytes caused liver failure, and the jaundice visible here and in an earlier photo.
Surface contour: elevation
A raised surface contour represents something added to the tissue. Raised surface contour may result from the presence of inflammatory cells, neoplastic cells, or hyperplastic cells. Tissues can also be expanded by the addition of water (edema), blood (hemorrhage, hematoma), air (emphysema) or other material.
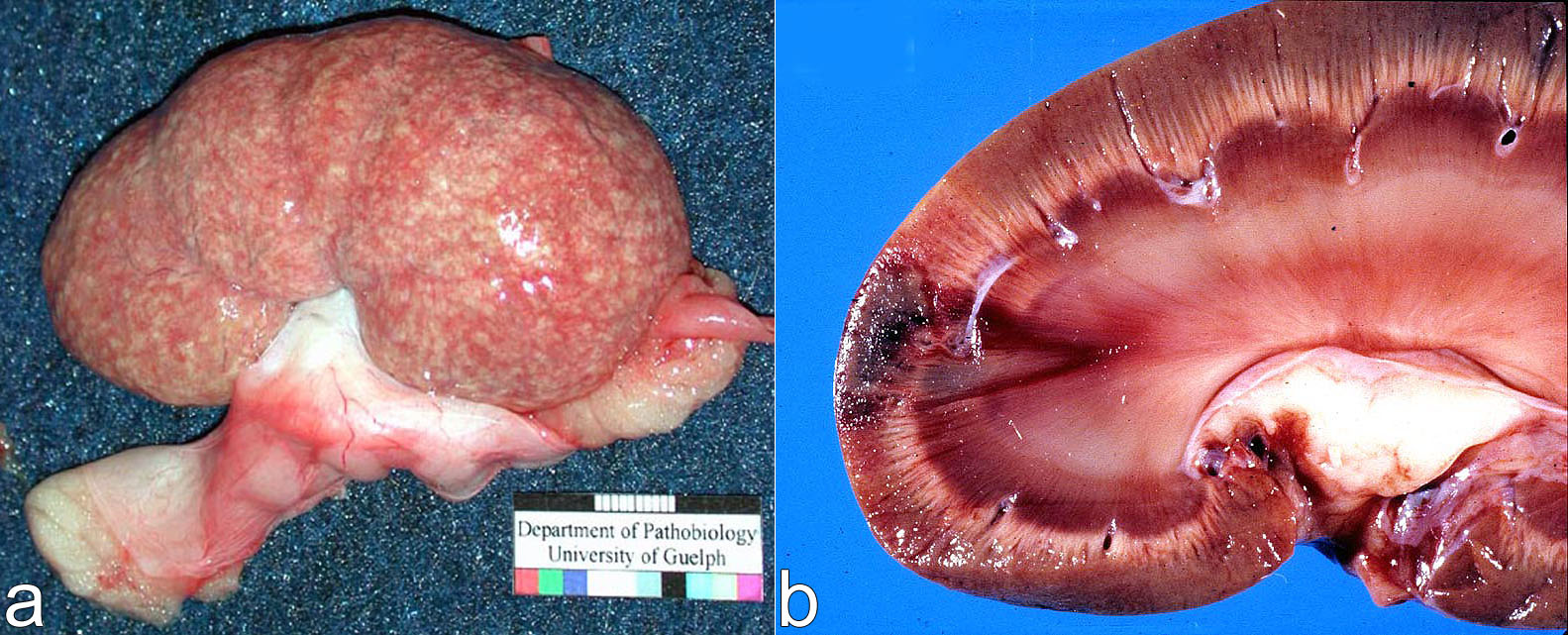
(a) Cat, kidney, feline infectious peritonitis (FIP). Mainly affecting the cortex, there are innumerable 0.5-4-mm-diameter soft tan foci that bulge from the capsular surface and the cut surface. These are foci of granulomatous inflammation, a form of inflammation that is not typical of virus infections generally, but is the characteristic lesion of FIP. The foci are raised because macrophages and other inflammatory cells are added to the tissue. (b) Cat, kidney. These well-demarcated tan nodules are metastases to the kidney from a distant primary tumor. The raised lesions are formed by proliferation of neoplastic cells (plus the accompanying connective tissue). Pale nodules are often the result of neoplasia, focal hyperplasia, or inflammation.
(a) Feedlot steer, esophageal mucosa, bovine papular stomatitis caused by parapox virus. The pale elevated edges of the lesions are virus-induced epithelial hyperplasia; the central depressions are due to virus-induced necrosis. Our gross observations tell us a lot about the underlying biology of this disease! (b) Dog, brain, granulomatous meningoencephalitis. The inflammation has caused brain edema which expands the brain tissue. But the brain is encased in the skull bones, so it is pushed into other cavities as it expands. Specifically, the occipital cortex (arrows) has squeezed over the tentorium cerebelli (like abdominal fat, hanging over a tight belt), and coning of the caudal part of the cerebellum as it is pushed through the foramen magnum into the spinal canal. This is an example of expansion of tissue due to edema.
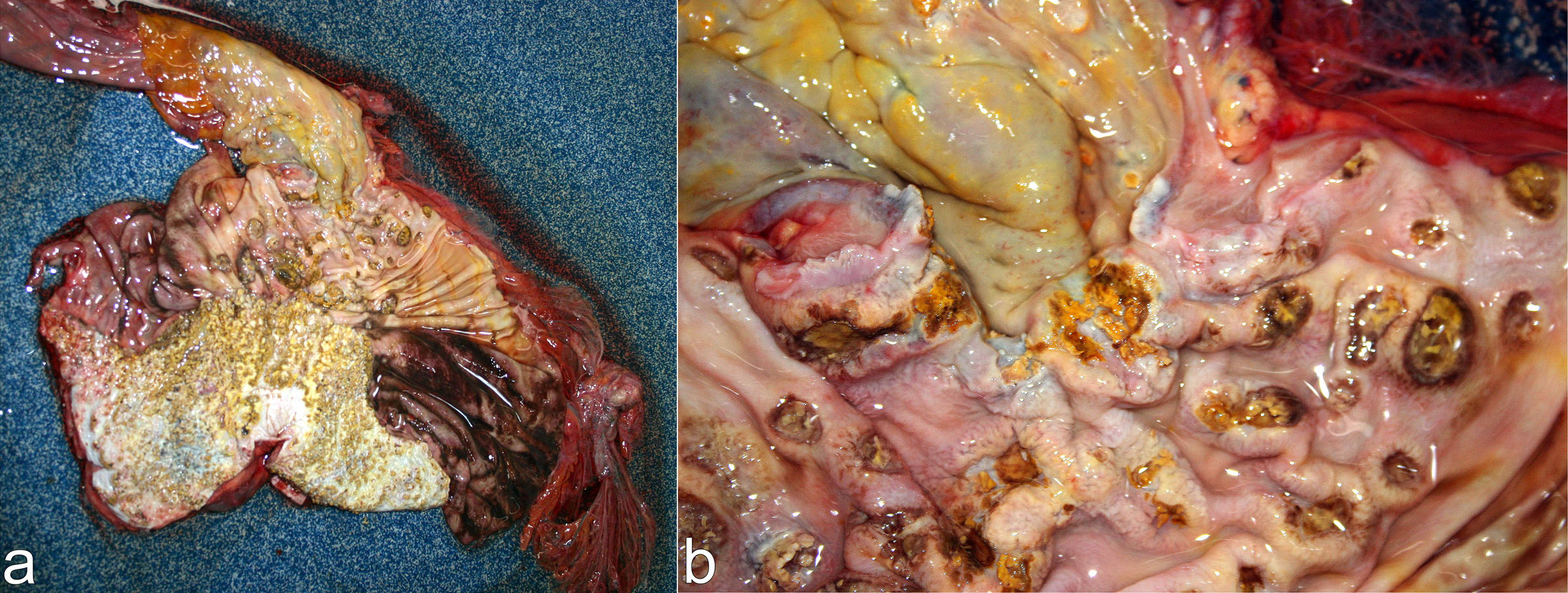
(a,b) Horse, opened stomach, “multisystemic eosinophilic epitheliotropic disease”. Lesions can be both raised and depressed! This gastric mucosa contains numerous expansile nodules that resulted from eosinophil infiltration. Necrosis and ulceration of the nodules has formed craters in the centre of the nodules. In this disease, eosinophils infiltrate various tissues in the body to form diffuse thickening or multiple nodules. The cause is unknown.
Colour: red
Mechanisms for accumulation of blood in tissues include hemorrhage, congestion, and hyperemia.
Above: Coalescing hemorrhages on the intestinal serosa, due to both thrombocytopenia and vascular damage. Dog, disseminated intravascular coagulation due to immune-mediated hemolytic anemia.
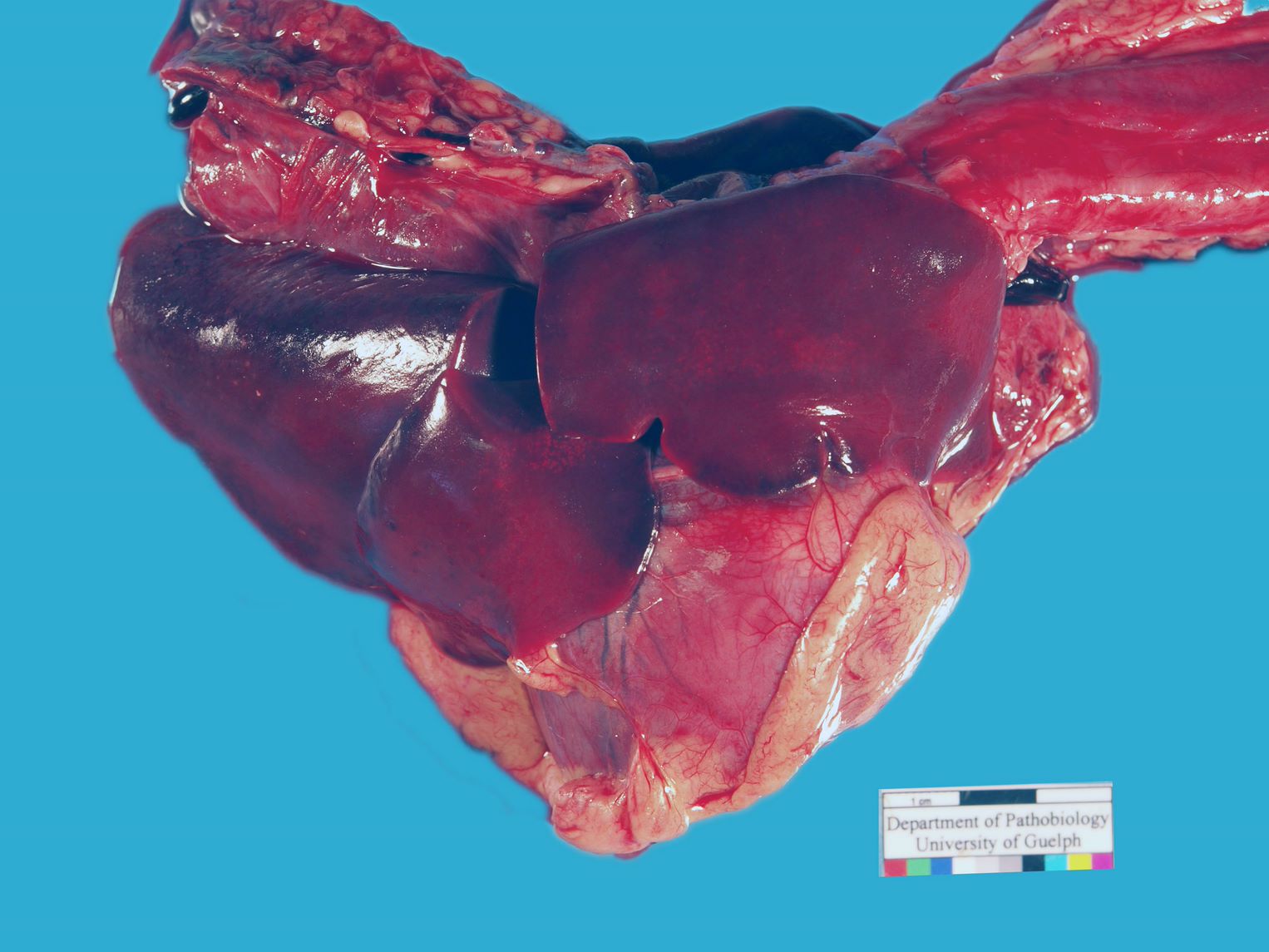
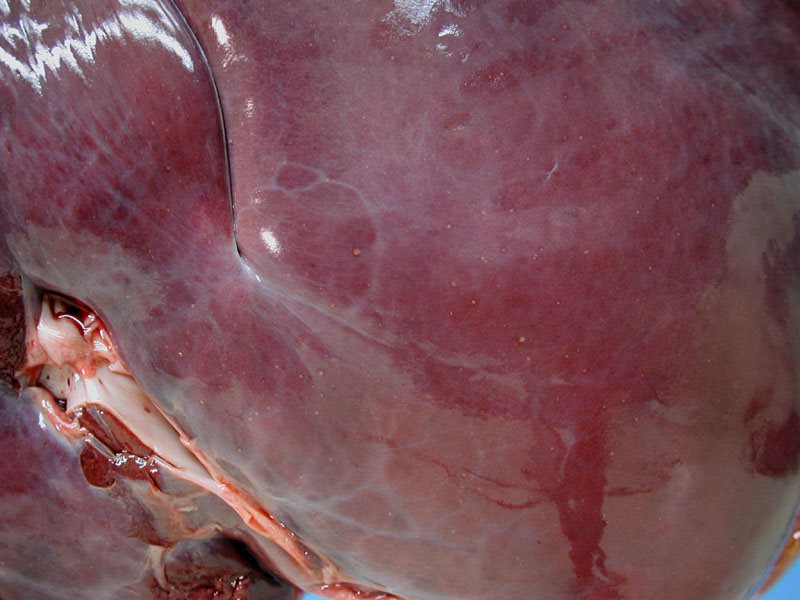
Above: Diffuse congestion of the liver due to right heart failure. Dog, anomaly causing obstruction of pulmonary blood flow.
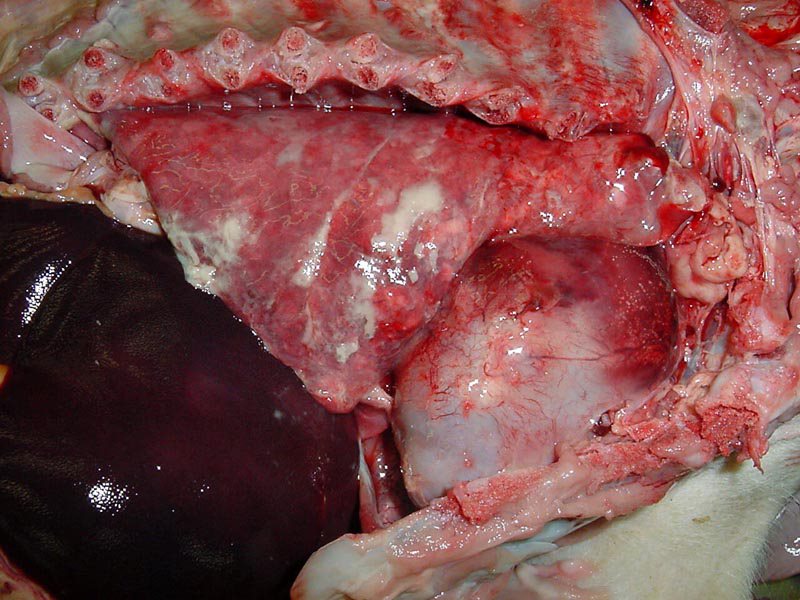
Right: Hyperemia due to inflammation, in the cranioventral area of lung. Calf, bronchopneumonia, Mannheimia haemolytica.
Hemorrhages are usually multifocal or patchy in distribution, whereas congestion or hyperemia are diffuse within the affected area. Extensive hemorrhage may, however, cause diffuse reddening. It is not possible to objectively distinguish congestion from hyperemia after death.
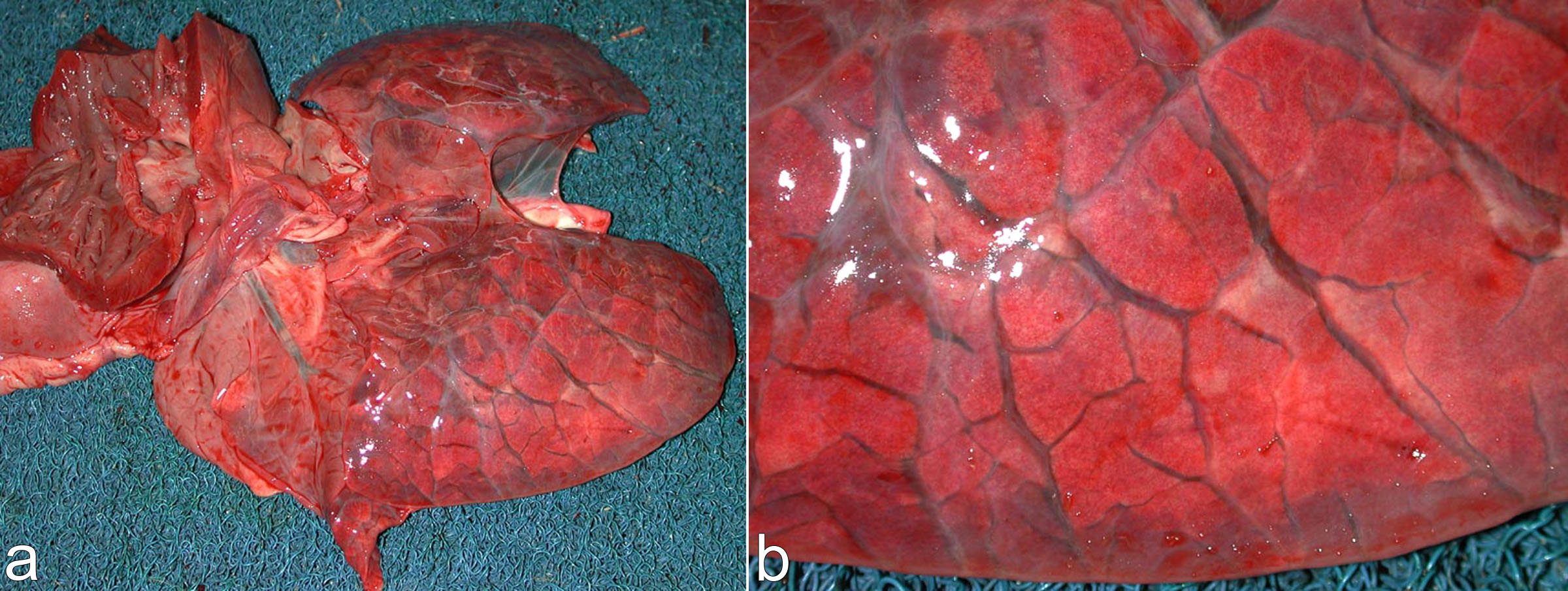
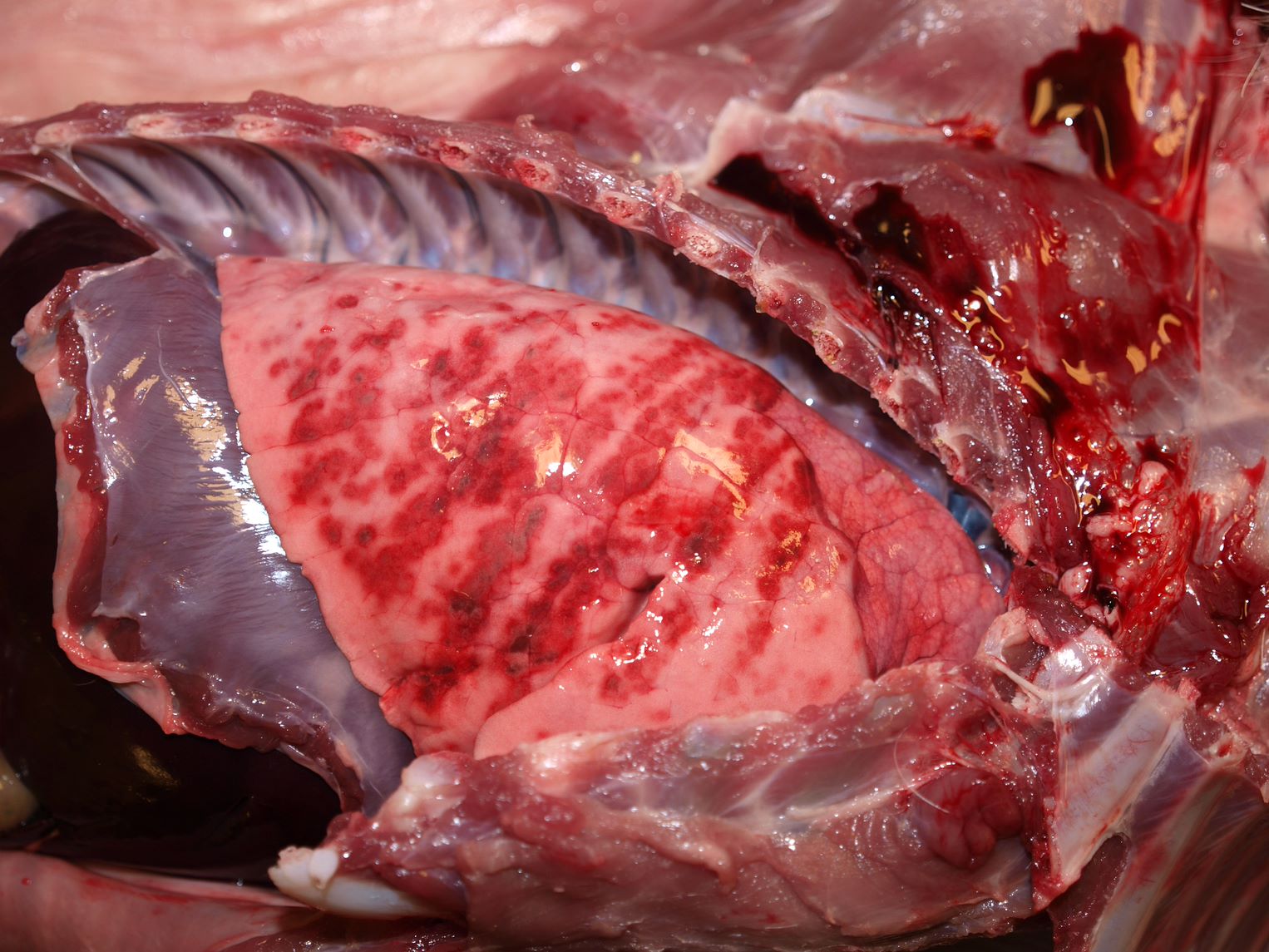
Above: Multifocal red lesions indicative of hemorrhages. Lamb, lung, vascular injury from Mannheimia haemolytica septicemia.
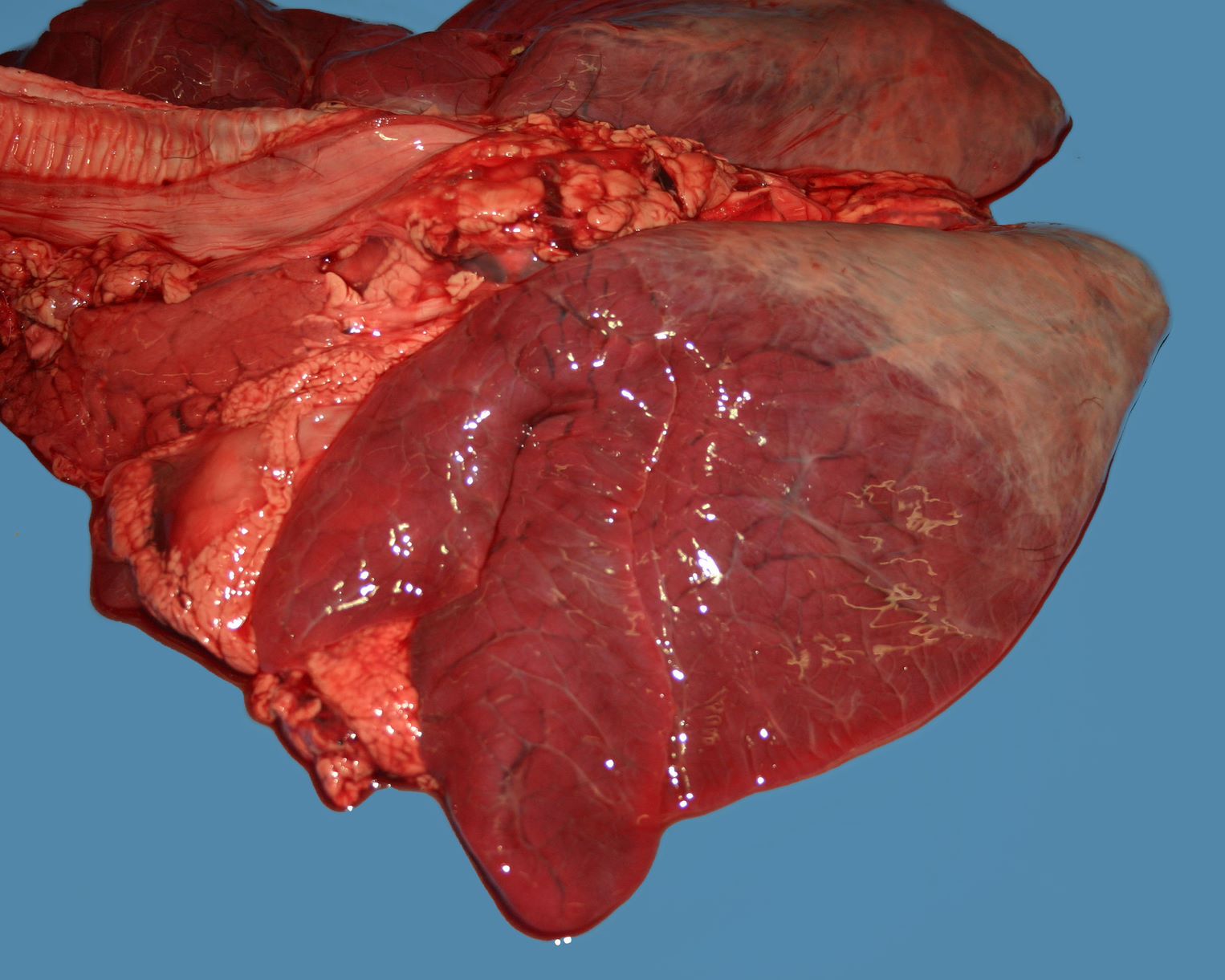
Above: Diffuse reddening due to congestion or hyperemia. Dog, lung, diffuse alveolar damage.
Two additional reasons for reddness.
Above: Aspiration of blood into the lung from the upper respiratory tract, at the time of euthanasia. Pig.
Below: Fetal atelectasis: the absence of air intensifies the inherent reddness of the lung.
Patterns of hemorrhage into infarcts.
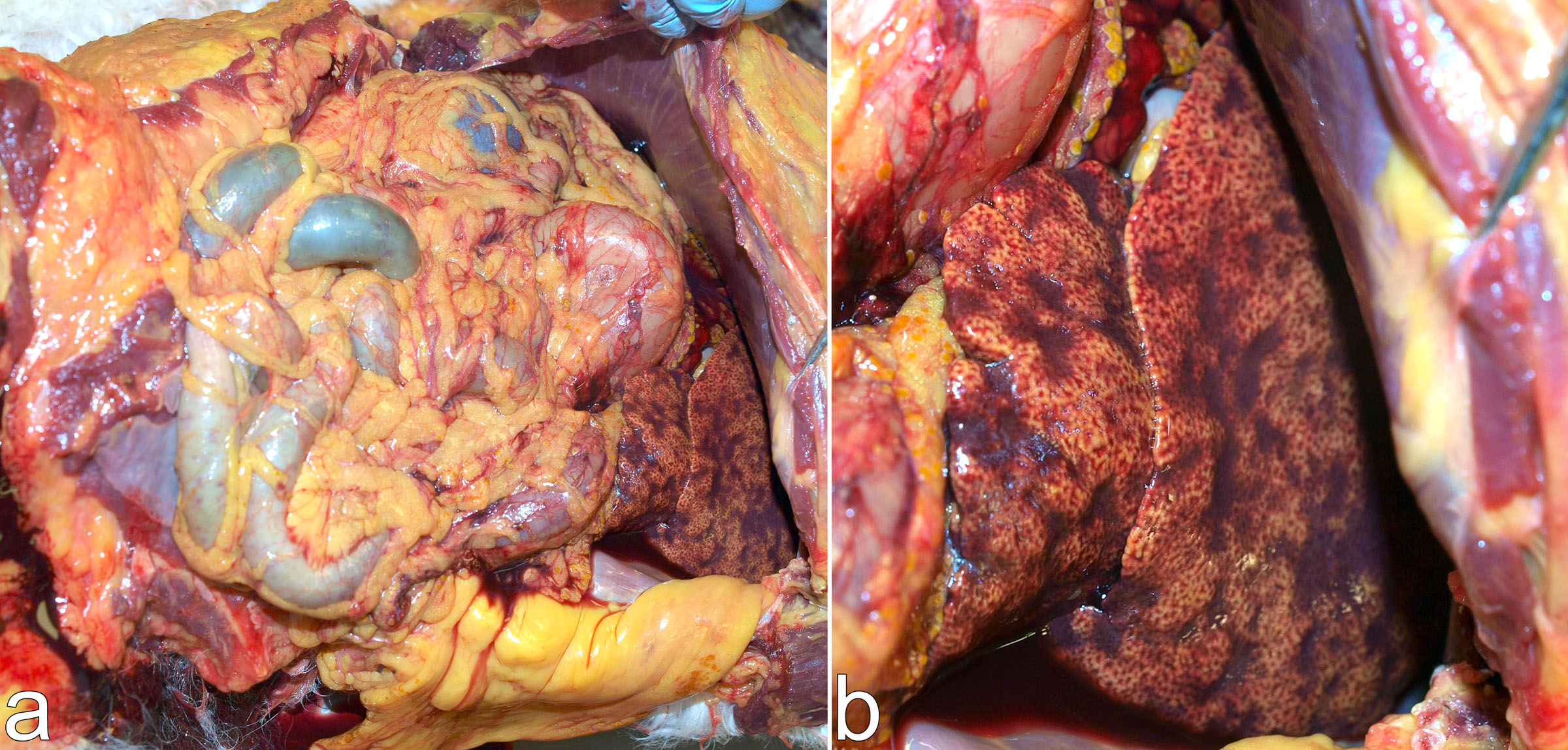
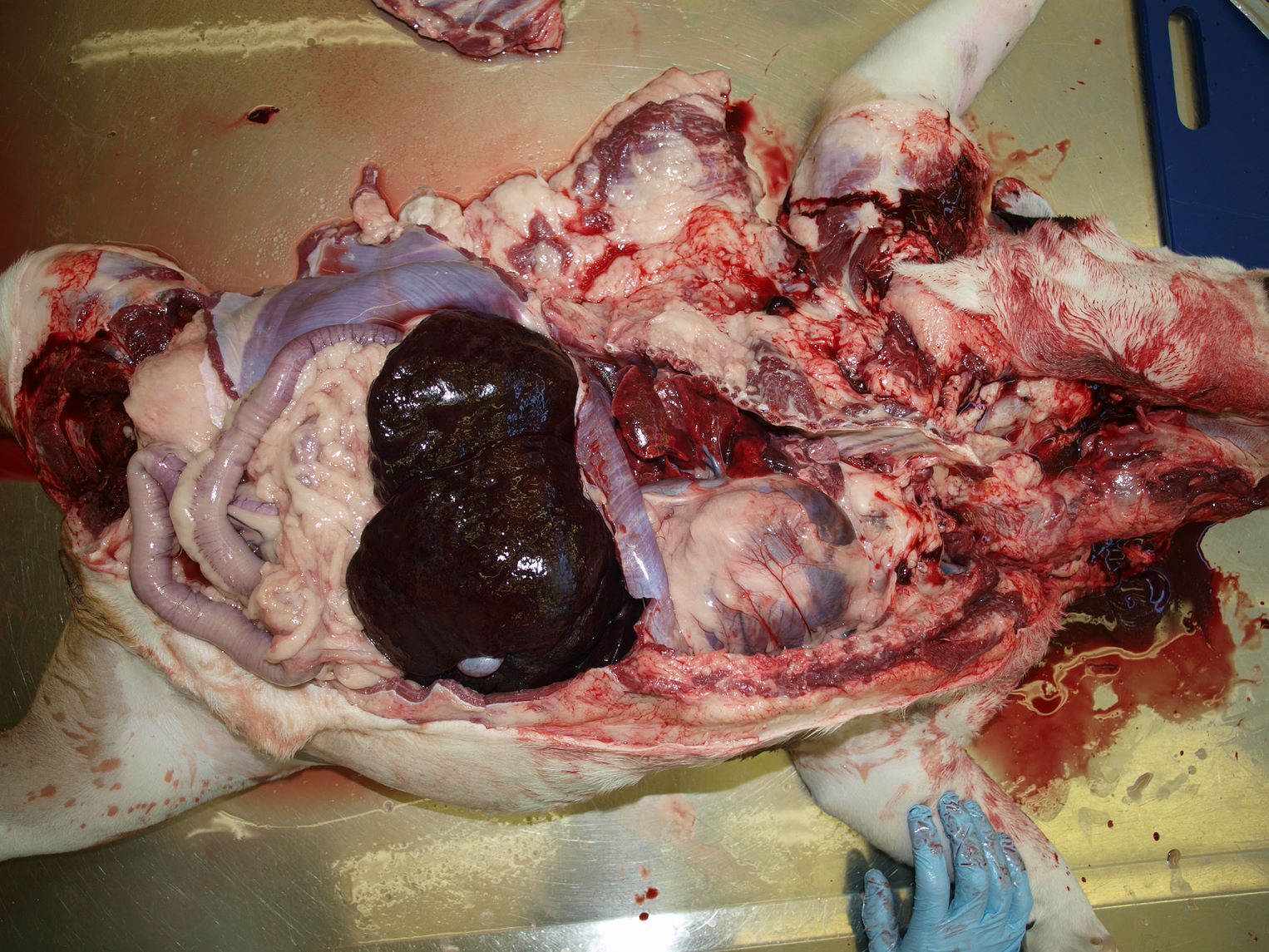
Above: In lung, spleen, liver and adrenal gland, arterial infarcts appear red because of hemorrhage into tissue spaces or sinusoids. Dog, lung, sepsis secondary to parvoviral enteritis.
Below: Arterial infarcts in most tissues appear pale, but may be delineated by a rim of hemorrhage. Dog, kidney.
Above: Blood fills the thoracic cavity, compressing the lungs. Note the pallor of the oral mucosa. Dog, Hemothorax due to anticoagulant rodenticide toxicity.
Below: Petechial hemorrhages from vascular damage. Horse, endotoxemia secondary to bacterial colitis.
Colour: tan and white
Causes of pale, tan or white lesions:
Addition of white cells: leukocytes (inflammation), neoplastic cells, epithelium. Lesions may be raised (or flat).
Addition of white substances: fibrin, fibrous tissue, mineral, lipid, glycogen, urate, nucleus pulposis
Cell swelling: tissue necrosis. Lesions may be depressed (or flat, or slightly raised), and friable (or of normal strength).
Removal of blood or other pigments: anemia, hypovolemia
Above: Kidney, septic infarct. Hemorrhage and necrosis, with white rim of leukocytes
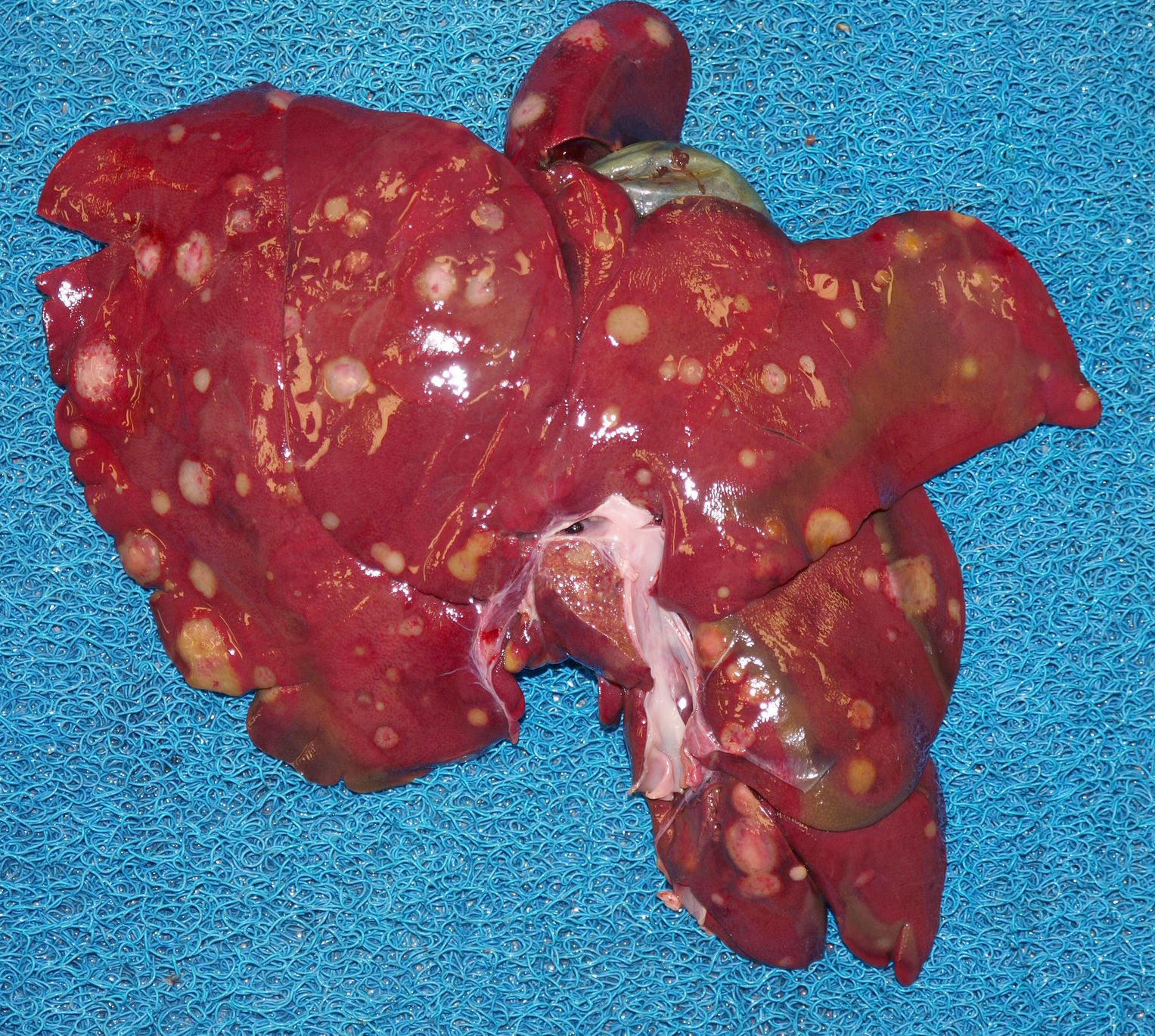
Above: Pale nodules in liver, which are metastatic sarcoma. Dog.
Above: Tan nodules of pyogranulomatous inflammation. Cat, kidney, FIP.
Above: Raised white rims of virus-induced epidermal hyperplasia. Piglet, pox virus.
Above: White fibrin on pleura. Pig, Haemophilus parasuis infection.
Above: White fibrin on pleura. Pig, Haemophilus parasuis infection.
Above: Urate crystals cover the epicardium. Falcon, visceral gout.
Above: Focus of pallor with a red margin: necrosis due to infarction, in the renal cortex. Horse, sepsis from bacterial colitis.
Above: Liver, aborted foal. Multiple white foci of necrosis caused by equine herpesvirus-1 infection.
Above: Dog. Pale oral mucosa due to anemia.
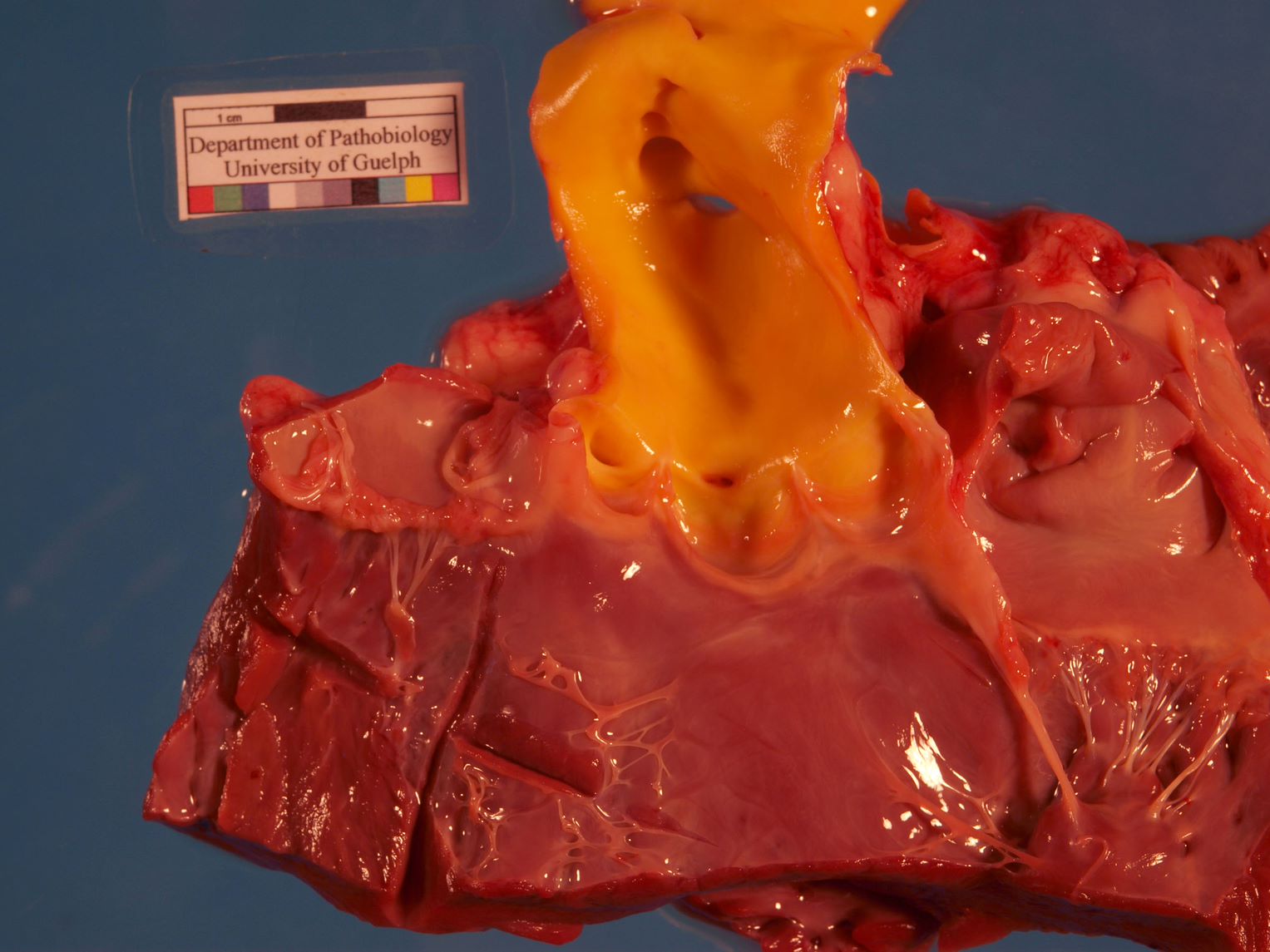
colour: yellow
Yellow discoloration of tissues usually represents bilirubin. This is most prominent in jaundice (icterus) as a result of hepatic disease, biliary obstruction, or hemolysis. Below are examples of mild and severe jaundice, in dogs with liver disease.
The subcutaneous and adipose tissues of horses are often slightly yellow, reflecting the normally higher levels of bilirubin in this species.
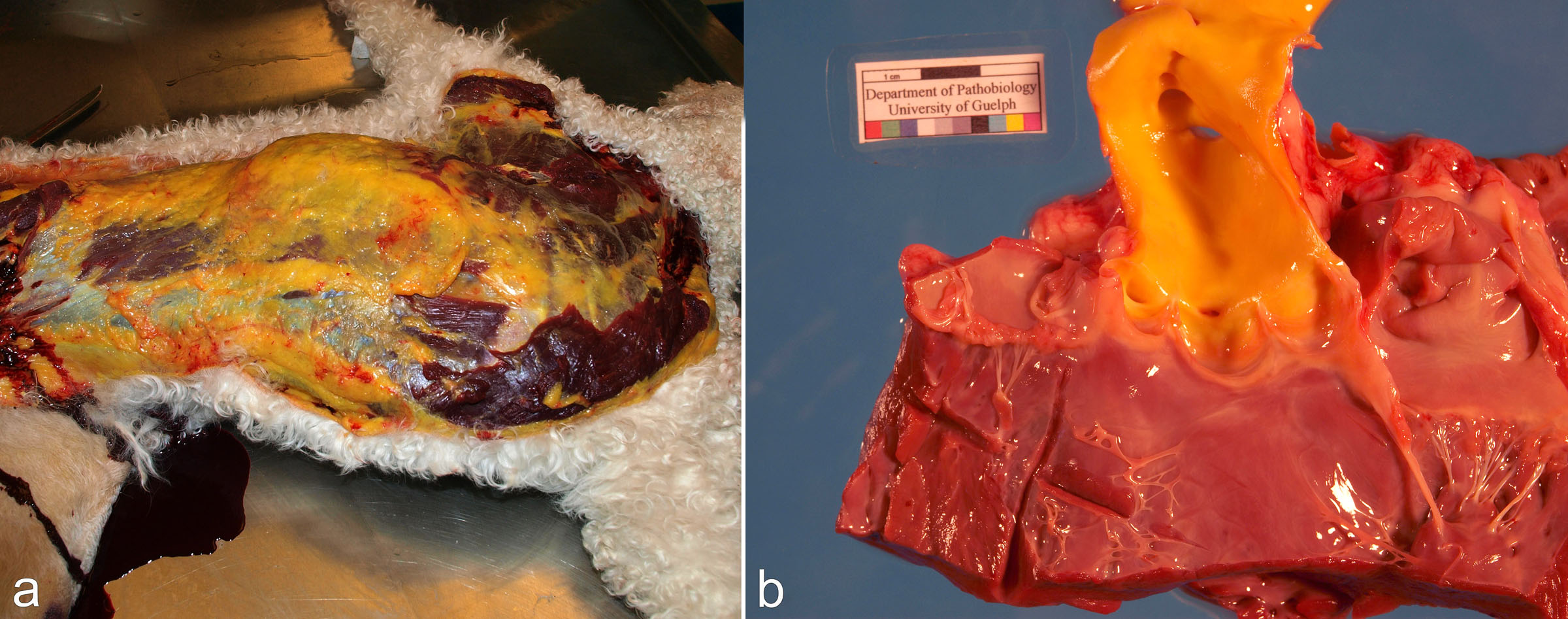
Edematous tissues and fibrin may be yellow, as is evident in the area of localized edema in the horse leg below.
colour: yellow & green
Green colour in fresh tissues may represent bile, or rarely eosinophils. Green or yellow discoloration is common near the gall bladder in autolysed carcasses. Putrefaction causes green discoloration of tissues after death.
Below: Dog, acute myeloid leukemia. Masses in lymph nodes and other tissues are obviously green, as a result of heme pigment in myeloperoxidase, an enzyme in the granules of the neoplastic myeloid cells.