Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Neurodiversity and Exceptionalities
Learning Objectives
Describe information processing and learning exceptionalities.
Summarize critiques of Piaget’s and Kohlberg’s theories.
Examine neurodiversity and learning exceptionalities.
Discuss how CYCs can support cognitive development in adolescence.
Introduction
Last week’s reading provided an overview of different types of learning, theories relating to cognitive development, and more context into how brain growth and development transform during adolescence. This reading goes over neurodiversity, exceptionalities in learning, reviews strength-based language, and the importance of this information to our work as CYCPs.
There are many diagnoses that fit into the category of neurodivergence, which are beyond the scope of this course. Many of these are covered in your Mental Health courses, so to keep our focus on development in adolescence, we will review terms in general and the relevance to our work with young people and families; links are included if you would like to learn more.
We have so far covered how the brain develops and grows during adolescence, now we are moving into learning about what the brain does with these advances. With the brain pruning connections and synapses (see previous readings and content) this creates more efficient retrieval of information, experiences, and allows for adolescents to apply their learning abstractly and think beyond the present, into the hypothetical.
Before we go into neurodiversity and exceptionalities, let’s look at how our brain stores and uses information.
Information-Processing Theories
How we think and process information varies from person to person. The information-processing perspectivederives from the study of artificial intelligence and explains cognitive development in terms of the growth of specific components of the overall process of thinking (Seifert & Sutton, 2009). Theories that focus on describing cognitive processes that underlie thinking at any one age and cognitive growth over time (Siegler, 2024). This is in contrast to Piaget’s stages of cognitive development, that are more linear and one must be achieved before the next. One of the main critiques of early cognitive theories is that achievement is lifelong, and always adapting and developing (Lumen Learning, 2019).
Improvements in basic thinking abilities generally occur in several areas during adolescence:
Attention: Improvements are seen in selective attention (the process by which one focuses on one stimulus while tuning out another), as well as divided attention (the ability to pay attention to two or more stimuli at the same time).
Memory: Improvements are seen in working memory and long-term memory.
Processing Speed: Adolescents think more quickly than children. Processing speed improves sharply between age five and middle adolescence, levels off around age 15, and does not appear to change between late adolescence and adulthood.
Organization: Adolescents are more aware of their own thought processes and can use mnemonic devices and other strategies to think and remember information more efficiently.
Metacognition: Adolescents can think about thinking itself. This often involves monitoring one’s own cognitive activity during the thinking process. Metacognition provides the ability to plan ahead, see the future consequences of an action, and provide alternative explanations of events.
Information-processing theories have become an influential alternative to Piaget’s approach. The theory assumes that even complex behaviour such as learning, remembering, categorizing, and thinking can be broken down into a series of individual, specific steps, and as a person develops strategies for processing information, they can learn more complex information. This perspective equates the mind to a computer, which is responsible for analyzing information from the environment.
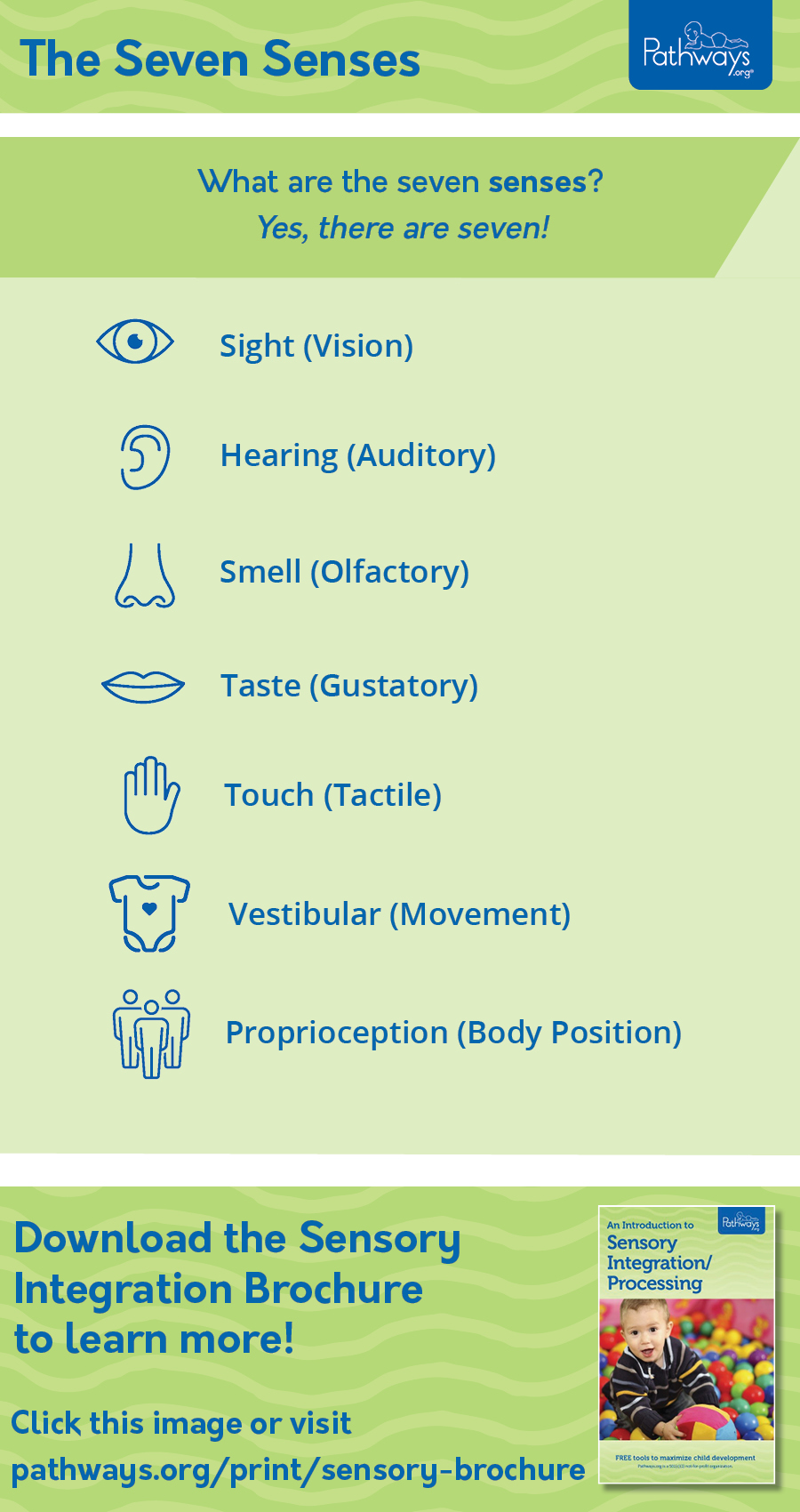
Image 1: A visual of the seven senses. Source: Pathways.org (2023)
Our brains are continuously taking information in, and we are many times unaware – meaning this is subconscious.
The information we take in comes from all the senses (see Figure 1). These include things we can:
See
Smell
Taste
Touch
Hear
There are also two senses relating to our body relating to:
Body movement
Body position
For more information on the senses and how we use them relating to development, visit: https://pathways.org/topics-of-development/sensory/ Note that this website looks at the early years of development, but consider how this processing of information continues into adolescence and emerging adulthood. What might this mean for us in terms of our work with young people and families? How can we use this information in our practice?
The ability to use the various senses is fundamental to the information processed by our brains, as these are the sensory inputs. Not having one or more of our senses available to us means that other senses are heightened (no, not our spidey-sense, unfortunately – and not quite to the extreme of someone like Daredevil… Again, that’s beyond the scope of this course!)
There are, however, exceptions to this – which we will explore later in this reading when we talk about sensory issues, which are a common theme for many learning exceptionalities and neurodivergent minds.
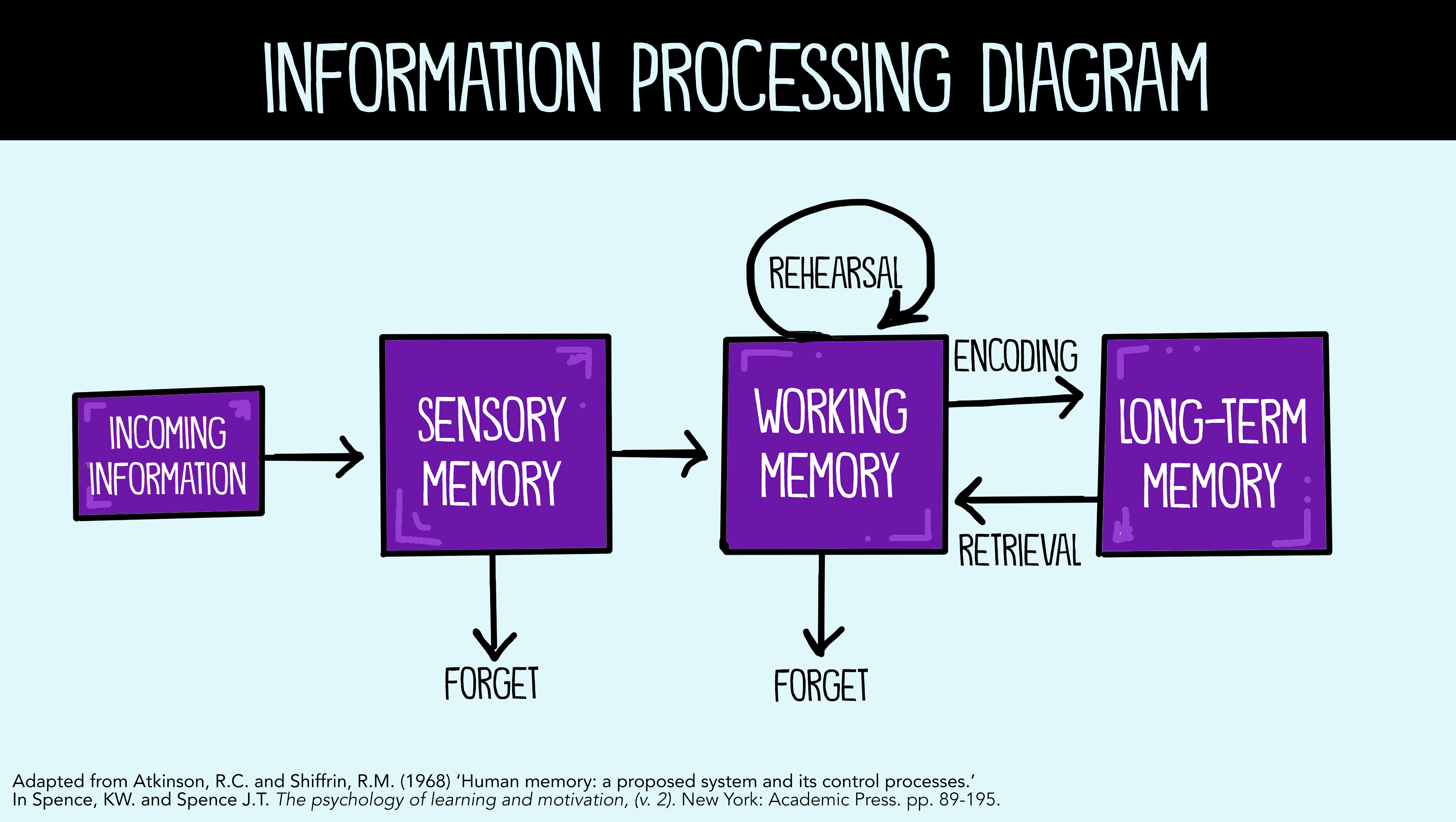
The most common information-processing model is applied to an understanding of memory and the way that information is encoded, stored, and then retrieved from the brain (Atkinson & Shiffrin, 1968), but information processing approaches also apply to cognitive processing in general. According to the standard information-processing model for mental development, the mind’s machinery includes attention mechanisms for bringing information in, working memory for actively manipulating information, and long-term memory for passively holding information so that it can be used in the future.
The graphic (Image 2) below provides a visual for how information is stored, accessed (or forgotten), and retrieved by the brain. Click the image to view a larger version in a new tab.
Image 2: Information Processing Diagram. Source: Spencer, J. T. (2020).
Cognitive control: As noted in earlier chapters, executive functions, such as attention, increases in working memory, and cognitive flexibility have been steadily improving since early childhood. Studies have found that executive function is very competent in adolescence. However, self-regulation, or the ability to control impulses, may still fail. A failure in self- regulation is especially true when there is high stress or high demand on mental functions (Luciano & Collins, 2012 as cited in Lally & Valentine-French, 2019). While high stress or demand may tax even an adult’s self-regulatory abilities, neurological changes in the adolescent brain may make teens particularly prone to more risky decision making under these conditions.
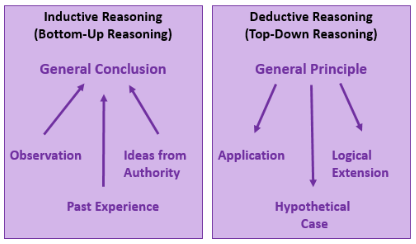
Inductive and Deductive Reasoning: Inductive reasoning emerges in childhood, and is a type of reasoning that is sometimes characterized as “bottom-up-processing” in which specific observations, or specific comments from those in authority, may be used to draw general conclusions. However, in inductive reasoning the veracity of the information that created the general conclusion does not guarantee the accuracy of that conclusion. For instance, a child who has only observed thunder on summer days may conclude that it only thunders in the summer. In contrast, deductive reasoning, sometimes called “top-down-processing”, emerges in adolescence. This type of reasoning starts with some overarching principle, and based on this propose specific conclusions. Deductive reasoning guarantees a truthful conclusion if the premises on which it is based are accurate.
Intuitive versus Analytic Thinking: Cognitive psychologists often refer to intuitive and analytic thought as the Dual-Process Model; the notion that humans have two distinct networks for processing information (Albert & Steinberg, 2011). Intuitive thought is automatic, unconscious, and fast (Kahneman, 2011, as cited in Lally & Valentine-French, 2019), and it is more experiential and emotional. In contrast, Analytic thought is deliberate, conscious, and rational. While these systems interact, they are distinct (Kuhn, 2013, as cited in Lally & Valentine-French, 2019). Intuitive thought is easier and more commonly used in everyday life. It is also more commonly used by children and teens than by adults (Klaczynski, 2001, as cited in Lumen Learning, 2019). The quickness of adolescent thought, along with the maturation of the limbic system, may make teens more prone to emotional intuitive thinking than adults.
The information-processing theory addresses how, as children grow, their brains likewise mature, leading to advances in their ability to process and respond to the information they received through their senses. The theory emphasizes a continuous pattern of development, in contrast with cognitive-developmental theorists such as Piaget, who thought development occurred in stages. Developmental psychologists who adopt the information-processing perspective account for mental development in terms of maturational changes in basic components of a child’s mind.
At the same time, they do not offer a complete explanation of behaviour. For example, they have paid little attention to behaviour such as creativity, in which the most profound ideas often are developed in a seemingly not logical, nonlinear manner.
Moreover, they do not take into account the social or cultural contexts (Alvares, 2011) in which development takes place! This applies to our work, as we approach development from a holistic perspective – taking into account every detail and context of a young person’s lifespace.
To understand more about how the brain can influence behaviour, and how we as CYCPs can go beyond the theories, let’s look at neurodiversity and exceptionalities.
Neurodiversity
Our societal expectations of how the brain functions is based on often outdated research, limited in most cases to studies on Eurocentric boys or men (Alvares, 2011). Researchers, mental health professionals, and the medical community tend to use a neurotypical expectation of how the brain works, and what we can be expected to do – in terms of functioning, thinking, and other areas. These are individuals “who’s functioning meets the dominant societal norms” (Wise, 2019). You will recall from your Mental Health course that the medical model “identifies mental differences as ‘abnormalities, disorders, deficits, or dysfunctions.’ From this perspective, some neurominority states are treated as medical conditions that can and should be corrected” (Disabled World, 2022).
Another definition by Oxford Languages (n.d.):
Θ neu·ro·typ·i·cal /ˌn(y)o͝orōˈtipikəl/
adjective
adjective: neurotypical; adjective: neuro-typical
not displaying or characterized by autistic or other neurologically atypical patterns of thought or behaviour.
“neurotypical individuals often assume that their experience of the world is either the only one or the only correct one”
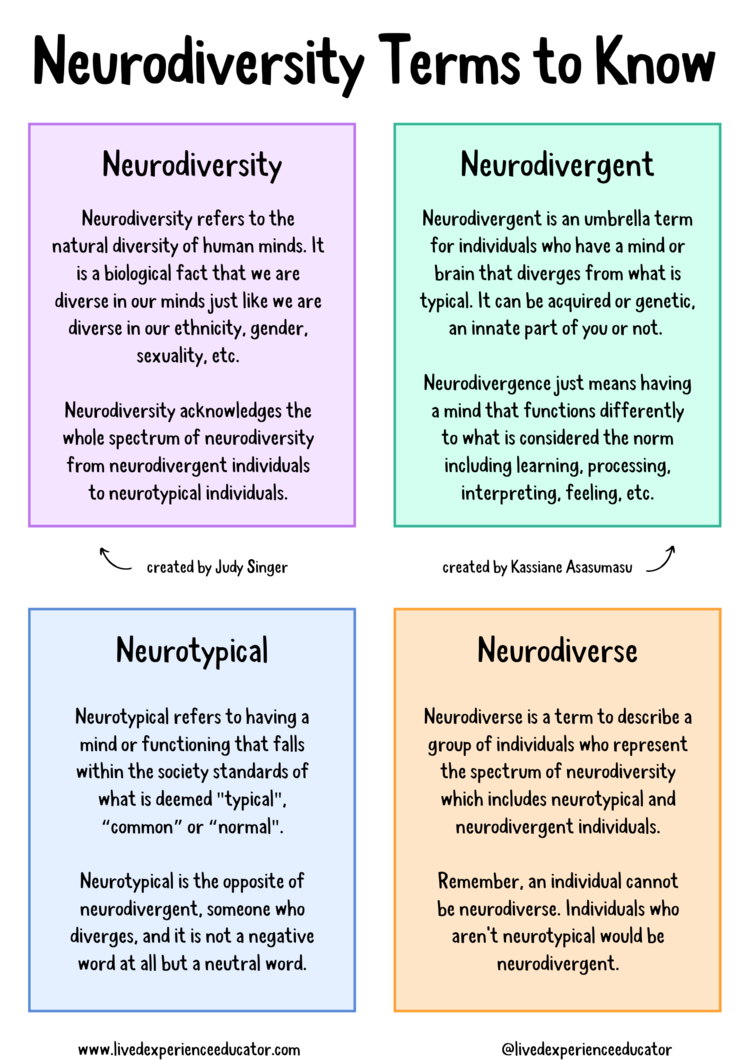
Current research is slowly becoming more inclusive, and this has allowed for a more thorough understanding of individual and natural differences in development, including what we know about the brain and how it is wired, known as neurodiversity (Child Mind Institute, 2024; Wise, 2019). This allows for different views of validating experiences, and not that there is a typical or expected way to think, or for brains to be wired. Image 4 highlights the various terms that are relevant to know, along with their differences:
Image 4: Neurodiversity Terms to Know from @livedexperienceeducator (2019)
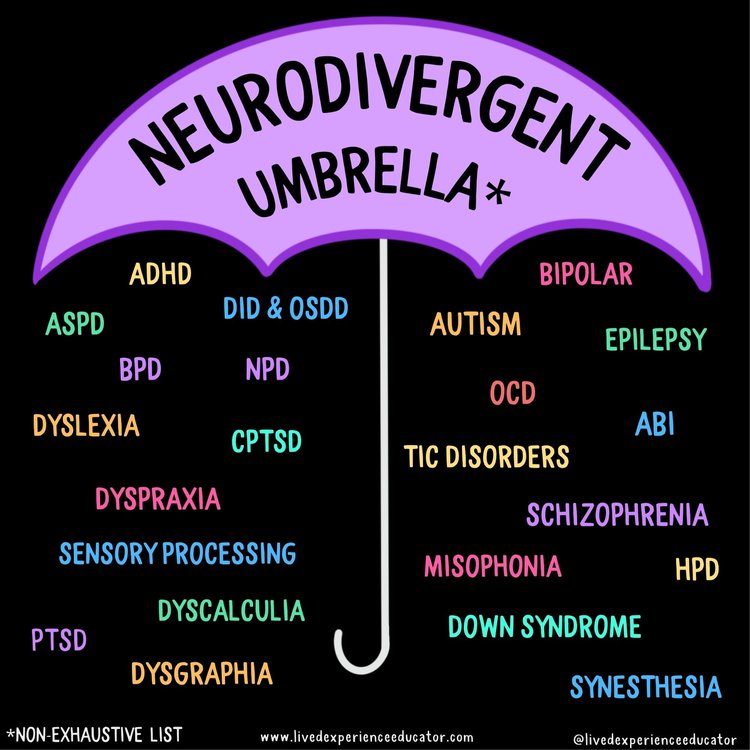
Image 5: A non-exhaustive list of what diagnoses are included in the neurodivergent umbrella.
Learning disabilities (LDs) and exceptionalities like the ones listed above can impact “the way in which a person takes in, remembers, understands and expresses information” (Learning Disabilities Association of Ontario, 2015 ). We will continue to learn about exceptionalities and neurodiversity throughout the program; consider this a brief introduction.
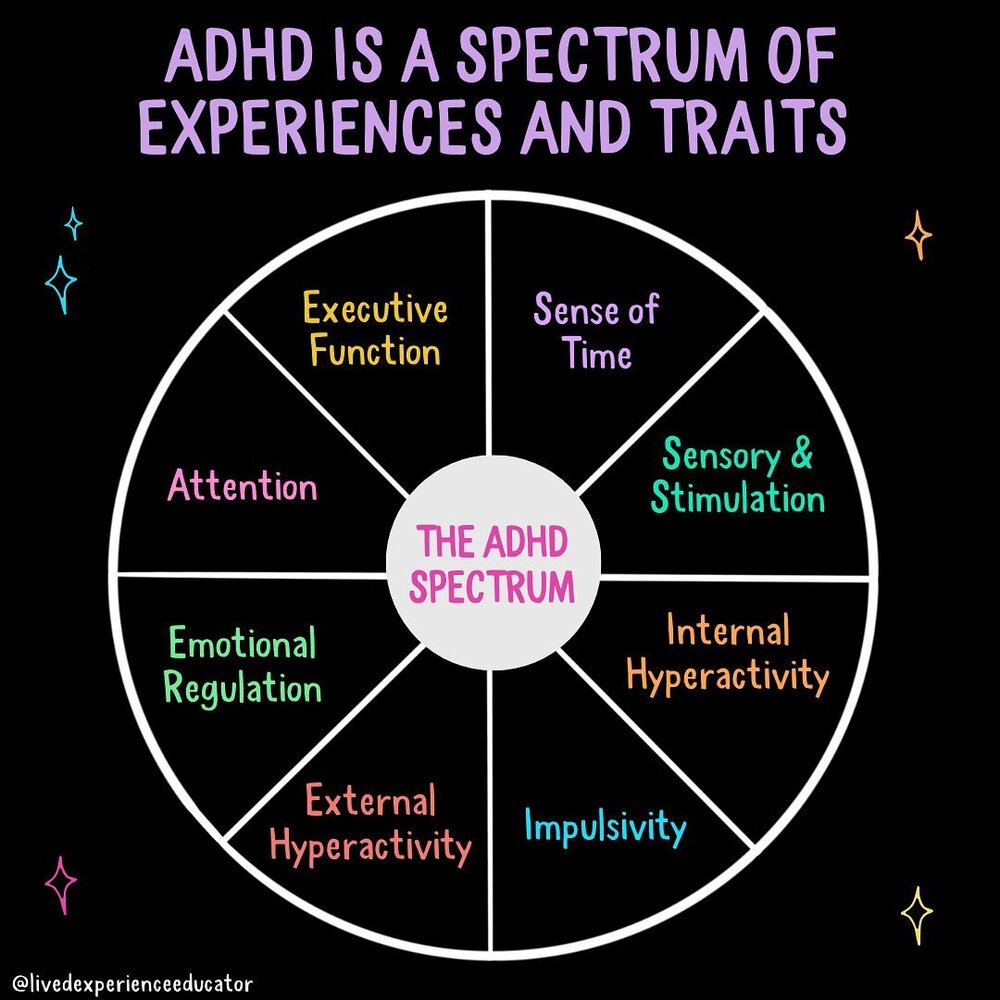
Many of these diagnoses exist on a spectrum – meaning individuals can have different traits and experiences- and others . For example, ADHD affects many areas of daily life as a result of how the brain is wired. Sees Images 6 and 7:
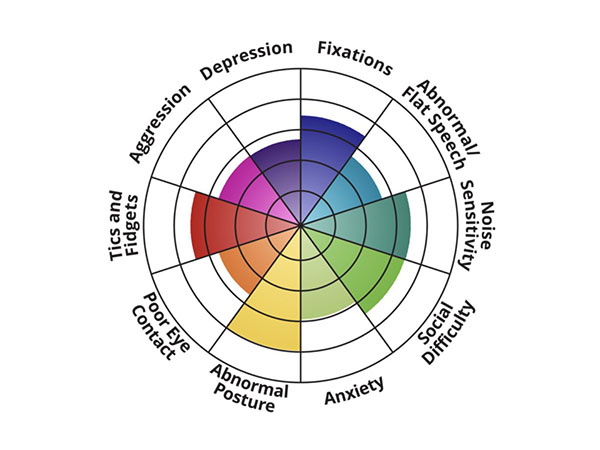
Image6: Depicting the ADHD spectrum of experiences and traits in a wheel which is unique to each person.Image 7: Depicting the autism spectrum of experiences and traits in a wheel, moving away from the concept of a spectrum.
Using a wheel to visually display the traits and experiences – many of which overlap between diagnoses – is moving away from the spectrum visual – which is more linear, general, and implies more or less impact overall, rather than looking at the different areas.
These two images demonstrate the different areas that are impacted by the diagnoses; which are assessed using criteria from the DSM 5: TR by a psychiatrist, psychologist, or other medical professional.
These are lifelong diagnoses, which one cannot outgrow – which some health professionals are still learning…
One of the main limitations of these assessments is the fact that the criteria used to confirm a diagnosis are historically based on research conducted using white, Eurocentric male participants. This has lead to late diagnoses and misdiagnoses for BIPOC, girls (assigned at birth). Individualized research expanding participant pools have started taking place in the last decade or two, leading to more inclusive criteria. Historically, too, diagnoses have little crossover – meaning the criteria for ADHD and Autism seldom overlap, and an individual may be diagnosed with one but not the other.
The emergence of social media has also increased awareness, however much information available is anecdotal, and creates blurred boundaries between experience and a formal diagnosis. Societal expectations on culture and gender also influence how an individual may behave, or display traits. One example is the lower rate of an ADHD diagnosis among girls (assigned at birth). “Girls with ADHD — especially those with inattentive symptoms — are often drowned out by loud, hyperactive boys who demonstrate the condition’s stereotypical behaviour” (Connolly, 2023). Boys (assigned at birth) are generally seen as more physical, and this behaviour is expected in many Western cultures. Girls (assigned at birth) are often expected to be quieter, sit still, and a girl with undiagnosed ADHD – or an individual who does not feel safe being or acting like themselves will ‘mask’ or hide behaviours, adding to the complexity of an accurate diagnosis, and often leading to misdiagnosis of another disorder (ADDitude, 2023).
Neurodiversity is one of the many populations we can support as a CYCP. Another category is that of exceptionalities. This term can include neurodiversity, but also includes other types as well.
For more information and descriptions of these and other types of neurodivergent minds, visit Exceptional Individuals’ website: Exceptionalindividuals.com and Childmind.org
Exceptionalities
Intelligence
Intellectual disability (or intellectual developmental disorder) is assessed based on cognitive capacity (IQ) and adaptive functioning. The severity of the disability is based on adaptive functioning, or how well the person handles everyday life tasks. About 1% of the United States population, most of them males, fulfill the criteria for intellectual developmental disorder, but some children who are given this diagnosis lose the classification as they get older and better learn to function in society. A particular vulnerability of people with low IQ is that they may be taken advantage of by others, and this is an important aspect of the definition of intellectual developmental disorder (Greenspan, Loughlin, & Black, 2001, as cited in Lally & Valentine-French, 2019).
Giftedness refers to those who have an IQ of 130 or higher (Lally & Valentine-French, 2019). Having an extremely high IQ is clearly less of a problem than having an extremely low IQ, but there may also be challenges to being particularly smart. It is often assumed that schoolchildren who are labeled as “gifted” may have adjustment problems that make it more difficult for them to create social relationships. To study gifted children, Lewis Terman and his colleagues (Terman & Oden, 1959, as cited in Lally & Valentine-French, 2019) selected about 1,500 high school students who scored in the top 1% on the Stanford-Binet and similar IQ tests (i.e., who had IQs of about 135 or higher), and tracked them for more than seven decades (the children became known as the “termites” and are still being studied today). This study found that these students were not unhealthy or poorly adjusted, but rather were above average in physical health and were taller and heavier than individuals in the general population. The students also had above-average social relationships and were less likely to divorce than the average person (Seagoe, 1975, as cited in Lally & Valentine-French, 2019).
Kids who are gifted have higher scores on general intelligence, but there are also different types of giftedness. Some children are particularly good at math or science, some at automobile repair or carpentry, some at music or art, some at sports or leadership, and so on. There is a lively debate among scholars about whether it is appropriate or beneficial to label some children as “gifted and talented” in school and to provide them with accelerated special classes and other programs that are not available to everyone. Although doing so may help some kids (Colangelo & Assouline, 2009, as cited in Lally & Valentine-French, 2019), it also may isolate them from their peers and make such access to resources unavailable to those who are not classified as “gifted.”
Exceptionalities in learning
In Ontario, the Ministry of Education (2022) recognizes five categories of exceptionalities :
Behaviour
Communication including Autism, Deaf and Hard of Hearing, Language Impairment and Learning Disability
Intellectual including Giftedness, Mild Intellectual Disability and Developmental Disability
Physical including Physical Disability and Blind and Low Vision
Multiple including Multiple Exceptionalities
A student in Ontario can be identified as ‘exceptional’ under any of these five categories of exceptionalities. “School Boards must develop an IEP for each ‘identified’ student and have the discretion to develop IEPs for students who are not identified as exceptional but are receiving special education services” [Fetal Alcohol Spectrum Disorder Ontario Network of Expertise (FASDONE), n.d.] Many diagnoses, such as FASD “can potentially touch on many, if not all, exceptionalities outlined by the Ministry” (FASDONE, n.d.).
“An exceptional pupil is a student who has behavioural, communicational, intellectual, physical or multiple exceptionalities that require them to have a special education program or service.” (Ontario Ministry of Education, 2022).
Community Living Ontario (2014) describes LDs as “brain-based difficulties that affect one or more ways that a person takes in, stores, recalls or uses verbal and nonverbal information. They are difficulties in processing information, and they occur in spite of average or above-average thinking and reasoning abilities.
LDs are not caused by environmental factors such as cultural differences or socio-economic status, although such factors can compound their impact.
LDs can interfere with learning basic skills such as reading, writing, and math. They can also interfere with higher-level skills such as organization, time management and social communication skills.”
Relevance to our work as Child and Youth Care Practitioners
Supporting individuals who have both an intellectual disability and a mental illness is rarely straightforward. Support work can be carried out by CYCPs, teachers, educational assistants, family members, or volunteers. Support can be offered in a variety of different environments including residential, educational, vocational, and recreation and leisure. In all aspects of support work, fundamental knowledge from the field of disability studies can offer caregivers important direction. This week’s content has been an introduction to this work, but there are courses and programs that go into much more detail!
Competencies Expected of support workers, CYCPs
What does it take to be informed and competent when supporting a young person, especially one who has a mental health, developmental, intellectual, or other exceptionality? A competency is an attribute, knowledge, skill, ability, or other characteristic that contributes to successful job performance. Competencies give rise to observable and measurable behaviours that contribute to individual success in an organization (e.g., teamwork and cooperation, communication). Child and Youth Care Practitioners, regardless of the service that is provided, require competencies in working with others, assessing strengths and needs, planning and providing services, linking to resources, advocacy, documenting and report writing, professionalism and ethical behaviour, and individualizing support requirements. See the Child and Youth Care Competencies, or revisit your textbook from Foundations in Child and Youth Care.
Working with othersis an expectation for direct support workers. The typical approach is to work collaboratively with others to plan and implement support plans. A multidisciplinary team might include professionals such as teachers, early childhood educators, psychologists, occupational therapists, physical therapists, medical professionals, and social workers. Parents, guardians, and family members are also integral to the team. Teams promote coordination and communication, and add to relationships. They may also identify service gaps and raise awareness of strategies, resources, and approaches that might be of benefit in direct support. Teams are extremely valuable in furthering positive outcomes for young people who are in difficult or complex situations.
Assessing strengths and needs is a significant part of the direct support worker’s job. The approach that is most favoured first identifies the talents, gifts, and skills of the individual being supported, with a view to using those to manage any needs the individual might have. An individualized strengths-based assessment then focuses on the complex interplay of risks and strengths among individual family members, the family as a unit, and the broader neighbourhood and environment. The individualized strengths-based approach is an overall philosophical view supported by policies and standards. It refers to practice methods and strategies that identify and draw upon the strengths of individuals, families, and communities.
Strengths-based practice requires a shift from a deficit approach, which emphasizes problems and pathology, to a positive approach (Rapp, Saleebey & Sullivan, 2005; Saleebey, 2006). A strengths-based approach values the capacity, skills, knowledge, connections, and potential in individuals and communities. Focusing on strengths does not mean ignoring challenges or spinning struggles into strengths. It does require that people work collaboratively.
Planning and providing servicesfollows assessing strengths and needs. Most services have adopted a person-centred process to assist people with disabilities and their families to build their capacities and capabilities. This planning effort is typically a series of discussions or interactions among the person with a disability, his or her family, and other members of the multidisciplinary team.
The team assists the individual in developing a description that includes a preferred place to live, favourite people with whom to socialize, and preferred types of daily activities, including preferred jobs. This description is based on the individual’s strengths, capabilities, preferences, lifestyle, and cultural background. The planning team decides what needs to be done, by whom, when, and how the individual is to work toward the preferred future. An individual program plan serves as a record of the decisions made by the planning team. This plan forms the foundation for the work of the direct service worker.
Linking to resourcesrequires the direct support worker to have comprehensive knowledge of the community in which the supported individual lives. Community asset mapping is one approach to acquiring this knowledge. The community asset mapping process (Asset Based Community Development Institute, n.d., as cited in Melrose, Dusome, Simpson, Crocker, & Athens, 2015) is intended to initiate full mobilization of a community and its assets around an individual vision. It allows mapping of relationships with other organizations for funding, referrals, access to resources, joint service planning, or collaborative projects with contributed staff. Once a community’s assets have been identified, the direct support worker is in a good position to begin linking the assets with the supported individual based on the individual’s strengths and needs.
Advocacyin all its forms seeks to ensure that people, particularly those who are most vulnerable in society, are able to have their voice heard on issues that are important to them. Advocacy supports and enables people to access information and services, defend and promote their rights and responsibilities, and explore choices and options (Support Empower Advocate Promote, n.d., as cited in Melrose et al., 2015).
The language we use when speaking with and about a young person is important. Recall your learning about strength-based language.
The name chosen to represent a disability (or exceptionality) has crucial implications for individuals to whom that name is applied. Therefore choose the name, term, or label with deliberate care. In the end, the name given to a disability should be able to meet the following standards (Luckasson & Reeve, as cited in Schalock & Luckasson, 2013):
The name should be specific and refer to a single disability. It should allow the disability to be differentiated from other disabilities.
The name should possess attributes that permit it to be accepted and used consistently by all stakeholders. Examples of stakeholders are individuals, families, service and support providers, professional organizations, advocacy groups, academics, researchers, government representatives, and policymakers.
The name should effectively represent the current state of knowledge and be able to integrate new knowledge as it appears.
The name should be functional in definition, diagnosis, classification, and planning of supports.
The name should have the capacity to communicate important values that are held for the named group of people.
People-First vs. Identity-First Language
Advocates, self-advocates, and professional groups generally agree that labels should not act as personal nouns to represent individuals (World Health Organization, 2002). For example, statements such as “Rashid is an epileptic” or “Maria is intellectually disabled” should be avoided. Individuals are much more than the disabilities they happen to experience. They are not defined by their disabilities. Instead, “people-first language” should be used to introduce the presence of disability. Statements such as “Rashid is a young man with (or, who has) epilepsy” or “Maria has Down Syndrome” or “Maria is a person who lives with intellectual disability” represent people-first language. Unless there is a reason to do so, mentioning an individual’s disability is not even needed. Consider how you might describe someone who does not have a disability: for example, “Rani has a very dry sense of humour” or “Ampreet has such a warm and caring manner” or “Sarah has a mischievous streak.”
This agreement that people-first language should frame conversations about intellectual disability extends to agreement that possessive language should be avoided when talking about conditions that are associated with intellectual or other disabilities. This means, for example, that the apostrophe and letter s should be removed when referring to Down’s syndrome. Down syndrome is, therefore, the terminology of choice (although some self-advocates prefer to say that they have Up syndrome). This avoids the paternalism in naming conditions, disorders, and diseases for the persons who first identified them. Another example is autism. Many individuals prefer the term ‘autistic’ over ‘person with autism’ – which is identity-first language. Read more at https://autisticadvocacy.org/about-asan/identity-first-language/
Implications for practice: Language to use
Key Points for CYCPs”
Use language that is respectful, caring, and kind, and that communicates that the person is valued.
Use language that is appropriate to age and culture. For example, when meeting an older adult, a common custom may be to use a greeting such as “I am pleased to meet you Mr. Dodge. May I call you Henry?” rather than presuming that Mr. Dodge can be called Henry simply because he has intellectual disability.
Use language that is preferred by the person living with the disability. For example, members of the People First self-advocacy organization in Great Britain prefer to say that they experience learning difficulties instead of saying that they have intellectual disability, or a learning disability.
Use the person’s name and discuss issues in the same way that you would discuss issues when talking with or talking about someone who does not live with intellectual disability.
Treat each person as a person first, and with the understanding that using diagnostic labels is required only rarely and only in highly specific situations.
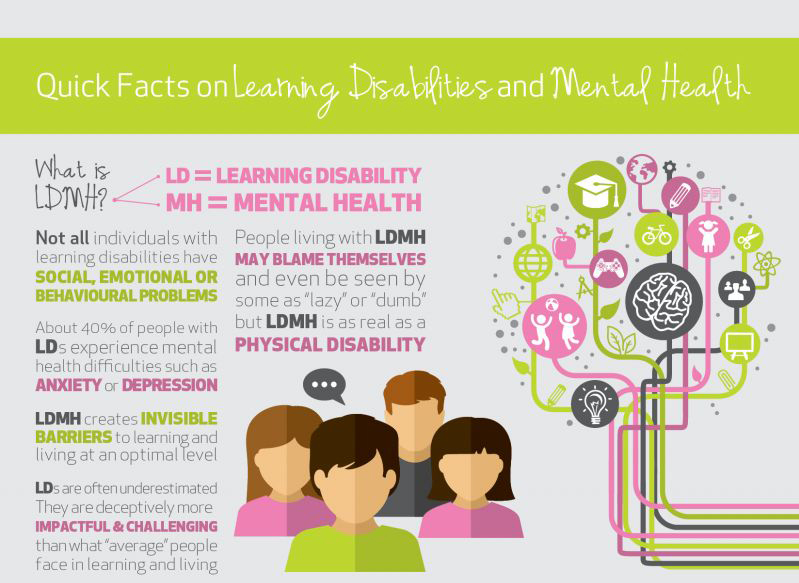
Child Development Institute (CDI, n.d), an accredited children’s mental health agency in Toronto, describes the following regarding LDs and mental health, but these stats are true of almost any exceptionality or neurodiversity:
Research indicates that 40 per cent of people with LDs are estimated to struggle with problems such as anxiety, depression or low self-esteem
75 per cent of children with LDs are estimated to have difficulties with social relationships
Depending on the nature of the LDs, it can be hard for these children to read social cues, adapt to new social situations or regulate their emotions or behaviours in order to fit in with peers
Children and youth who have LDs may experience feelings of frustration, shame and perceived stigma, hopelessness and anxiety about not meeting expectations
Kids with LDs are at greater risk for bullying and victimization, social isolation and rejection or feelings of loneliness
Regardless of the diagnosis, needs, etc., the more context we have about an individual, the more we know about them, and the stronger our relationship, the better we can support and adapt.
Intensities of support needs are classified as intermittent, limited, extensive, and pervasive. For any individual, these may vary from domain to domain and from time to time, depending on events and circumstances. Intensities of support needs are described as follows:
Intermittent. Support is periodic and of short duration. An example is support during lifespan transitions such as job loss, family member loss, or an acute medical crisis. During the time that it is given, this support may be of high or low intensity.
Limited. Support is more consistent but not intense. An example of this support is time-limited employment training.
Extensive. Regular support (e.g., daily) is provided in some environments. For example, long-term support may be required in the home or work environments.
Pervasive. Intense and constant supports are provided in all environments. These supports have life-sustaining potential, and typically involve more staff members and intrusiveness than extensive or limited supports. Keep in mind, however, that intermittent supports may be high intensity during the time that they are provided (Luckasson et al., 2002).
Link to Learning
Knowing what you now know about the brain and how it develops (and all the unique differences!) take a moment to explore these resources to learn more about accommodations, modifications, and how we can adapt and be inclusive in our practice with adolescents.
The way we as CYCPs support cognitive development, are inclusive in our approach and practice, and understand the needs of the adolescents we work with all become important when working with exceptionalities, disabilities, and neurodivergence. In practice, in our language, through our interventions, activities, accommodations we support and advocate for, we can adapt and be inclusive of any individual’s needs.
This week’s reading has been an overview – there’s so much more information out there!
Connolly, M. (2023). Girls with ADHD — especially those with inattentive symptoms — are often drowned out by loud, hyperactive boys who demonstrate the condition’s stereotypical behavior. ADDitude. Retrieved from https://www.additudemag.com/adhd-in-girls-women/
Luckasson, R., Borthwick-Duffy, S., Buntinx, W.H.E., et al., (2002). Mental Retardation: Definition, classification, and systems of supports (10th ed.). Washington, DC: American Association on Mental Retardation.
Luckasson, R. & Reeve, A. (2001). Naming, defining, and classifying in mental retardation. Mental Retardation, 39(1), 47–52. doi:10.1352/0047-6765(2001)039<0047:NDACIM>2.0C);2
Rapp, C. A., Saleebey, D., & Sullivan, W. P. (2005). The future of strengths-based social work. Advances in Social Work, 6(1), 79–90.
Saleebey, D. (2006). The strengths perspective in social work practice (4th ed.). Boston: Allyn & Bacon.
Schalock, R.L. & Luckasson, R. (2013). What’s at stake in the lives of people with intellectual disability? Part I: The power of naming, defining, diagnosing, classifying, and planning supports. Journal of Intellectual and Developmental Disabilities, 51(2), 86–93. doi:10.1352/1934-9556-51.2.086
World Health Organization (2002). Towards a common language for functioning, disability and health. The International Classification of Functioning, Disability and Health. Geneva, Switzerland. Retrieved from http://www.who.int/classifications/icf/training/icfbeginnersguide.pdf
OER Attributions:
Content from this chapter has been adapted from the following sources: