Genetic Bases of Development, Prenatal Development and Birth
Chapter Objectives
After this chapter, you should be able to:
- Examine the mechanisms of heredity and genetic disorders
- Define elements of nature and nurture
- Describe the influence of nutrition and stress on development
- Examine teratogens and their impact on prenatal development
Introduction
We will begin by examining some of the ways in which heredity helps to shape the way we are. We will look at what happens genetically during conception, and describe some known genetic and chromosomal disorders. Next, we will consider what happens during prenatal development, including the impact of teratogens, nutrition, and stress.
This aspect of development is an important one for caregivers, CYCPs, educators, and other professionals to consider. The Ontario Association of Child and Youth Care (OACYC, 2017) have two elements of the Code of Ethics that highlight this importance:
I. Responsibility for self
B. Develops knowledge and skills necessary to benefit children, youth, and families
II. Responsibility to children, youth and families
C. Ensures services are culturally sensitive and non-discriminatory (regardless of race, colour, ethnicity, national origin, national ancestry, age, gender, sexual orientation, marital status, religion, mental or physical capacity/ability, medical condition, political views, or socioeconomic status)
Last week’s reading described the ‘Applied Human Development‘ Domain of Practice for professional CYCPs. The foundational knowledge is as follows:
A. Foundational Knowledge
The professional practitioner is well versed in current research and theory in human development with an emphasis on a developmental-ecological perspective.
- Lifespan human development
- Child and adolescent development as appropriate for the arena of practice, (including domains of cognitive, social-emotional, physiological, psycho-sexual, and spiritual development)
- Exceptionality in development (including at-risk and special needs circumstances such as trauma, child abuse/neglect, developmental psychopathology, and developmental disorders)
- Family development, systems and dynamics
As you can see, our understanding of development includes the lifespan. This week, we look at what takes place prior to and at conception, as well as at birth. Next week we will explore physical development in more detail, but for now this is a good start.
Heredity, Nature & Nurture
Most scholars agree that there is a constant interplay between nature (heredity) and nurture (the environment). It is difficult to isolate the root of any single characteristic as a result solely of nature or nurture, and most scholars believe that even determining the extent to which nature or nurture impacts a human feature is difficult to answer. In fact, almost all human features are polygenic (a result of many genes) and multifactorial (a result of many factors, both genetic and environmental). It’s as if one’s genetic make-up sets up a range of possibilities, which may or may not be realized depending upon one’s environmental experiences. For instance, a person might be genetically predisposed to develop diabetes, but the person’s lifestyle may determine whether or not they actually develop the disease.
It may seem obvious that we are born with certain characteristics while others are acquired, and yet of the three great questions about humans’ relationship with the natural world, only nature–nurture gets referred to as a “debate.” In the history of psychology, no other question has caused so much controversy and offense: We are so concerned with nature–nurture because our very sense of moral character seems to depend on it. While we may admire the athletic skills of a great basketball player, we think of his height as simply a gift, a payoff in the “genetic lottery.” For the same reason, no one blames a short person for his height or someone’s congenital disability on poor decisions: To state the obvious, it’s “not their fault.” But we do praise the concert violinist (and perhaps her parents and teachers as well) for her dedication, just as we condemn cheaters and bullies for their negative behaviour.
The problem is, most human characteristics aren’t usually as clear-cut as height or instrument-mastery, affirming our nature–nurture expectations strongly one way or the other. In fact, even the great violinist might have some inborn qualities—perfect pitch, or long, nimble fingers—that support and reward her hard work. And the basketball player might have eaten a diet while growing up that promoted his genetic tendency for being tall. When we think about our own qualities, they seem under our control in some respects, yet beyond our control in others. And often the traits that don’t seem to have an obvious cause are the ones that concern us the most and are far more personally significant.
Some common questions about nature–nurture are, how susceptible is a trait to change, how malleable is it, and do we “have a choice” about it? These questions are much more complex than they may seem at first glance (Turkheimer, 2023).

This bidirectional interplay between nature and nurture is the epigenetic framework, which suggests that the environment can affect the expression of genes just as genetic predispositions can impact a person’s potentials. And environmental circumstances can trigger symptoms of a genetic disorder (Lumen Learning, n.d.).
Epigenetics
Epigenetics is “the study of heritable changes in gene expression or cellular phenotype caused by mechanisms other than changes in the underlying DNA sequence” (Weaver, 2023). Epigenetic studies have the potential to provide answers to these important questions and refers to the transmission of phenotype in terms of gene expression in the absence of changes in DNA sequence—hence the name epi- (Greek: επί- over, above) genetics (Waddington, 1942; Wolffe & Matzke, 1999).
The advent of high-throughput techniques such as sequencing-based approaches to study the distributions of regulators of gene expression throughout the genome led to the collective description of the “epigenome.” In contrast to the genome sequence, which is static and the same in almost all cells, the epigenome is highly dynamic, differing among cell types, tissues, and brain regions (Gregg et al., 2010 as cited in Pye, Scoffin, Quade & Krieg, 2022).
Recent studies have provided insights into epigenetic regulation of developmental pathways in response to a range of external environmental factors (Dolinoy, Weidman, & Jirtle, 2007, as cited in Lumen Learning (n.d.). These environmental factors during early childhood and adolescence can cause changes in expression of genes conferring risk of mental health and chronic physical conditions. Thus, the examination of genetic–epigenetic–environment interactions from a developmental perspective may determine the nature of gene misregulation in psychological disorders.
Genes and Chromosomes
Now, let’s look more closely at just nature. Nature refers to the contribution of genetics to one’s development. The basic building block of the nature perspective is the gene. Genes are recipes for making proteins, while proteins influence the structure and functions of cells. Genes are located on the chromosomes and there are an estimated 20,500 genes for humans, according to the Human Genome Project (NIH, 2015, as cited in Paris, Ricardo, Raymond, & Johnson, 2021).
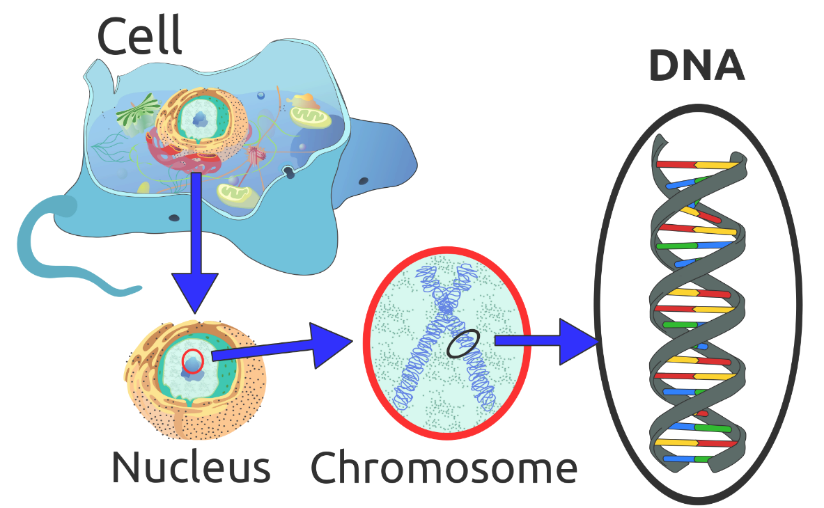
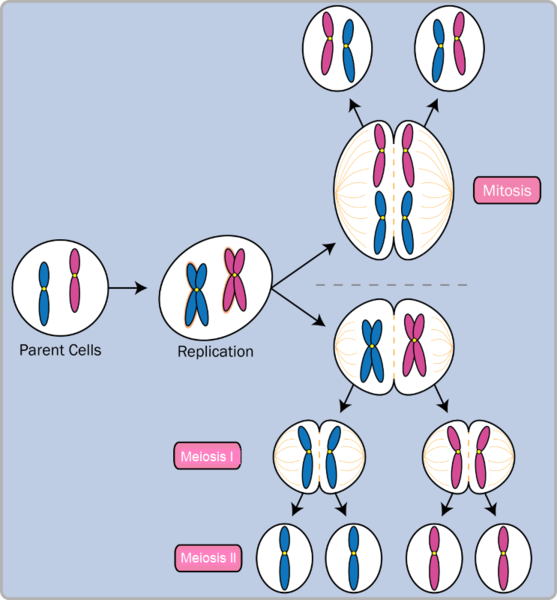
Normal human cells contain 46 chromosomes (or 23 pairs; one from each parent) in the nucleus of the cells. After conception, most cells of the body are created by a process called mitosis. Mitosis is defined as the cell’s nucleus making an exact copy of all the chromosomes and splitting into two new cells.
However, the cells used in sexual reproduction, called the gametes (sperm or ova), are formed in a process called meiosis. In meiosis, the gamete’s chromosomes duplicate, and then divide twice resulting in four cells containing only half the genetic material of the original gamete. Thus, each sperm and egg possesses only 23 chromosomes and combine to produce the normal 46.
| Type of Cell Division | Explanation | Steps |
| Mitosis | All cells, except those used in sexual reproduction, are created by mitosis | Chromosomes make a duplicate copy
Two identical cells are created |
| Meiosis | Cells used in sexual reproduction are created by meiosis | Exchange of gene between the chromosomes (crossing over)
Chromosomes make a duplicate First cell division Second cell division |
Table 1: Mitosis & Meiosis (Lally & Valentine-French, 2019).
Given the number of genes present and the unpredictability of the meiosis process, the likelihood of having offspring that are genetically identical (and not twins) is one in trillions (Gould & Keeton, 1997, as cited in as cited in Paris et al., 2021).
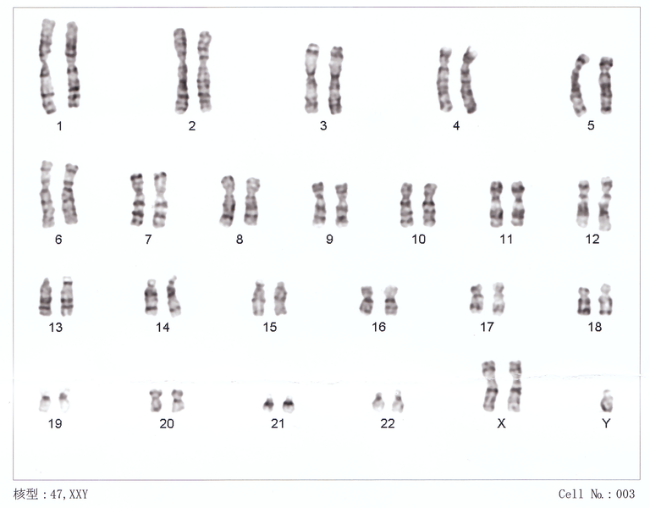
Of the 23 pairs of chromosomes created at conception, 22 pairs are similar in length. These are called autosomes. The remaining pair, or sex chromosomes, may differ in length. It is the Y chromosome that determines sex. If the Y chromosome is present, the child will be genetically male. If the Y chromosome is absent, the child will be genetically female (Lally & Valentine-French, 2019).
Here is an image (called a karyogram) of what the 23 pairs of chromosomes look like. Notice the differences between the sex chromosomes in female (XX) and male (XY).
Genotypes, Phenotypes & Patterns on Inheritance
The word genotype refers to the sum total of all the genes a person inherits. The word phenotype refers to the features that are actually expressed. Look in the mirror. What do you see, your genotype or your phenotype? What determines whether or not genes are expressed?
Because genes are inherited in pairs on the chromosomes, we may receive either the same version of a gene from our mother and father, that is, be homozygous for that characteristic the gene influences. If we receive a different version of the gene from each parent, that is referred to as heterozygous.
In the homozygous situation we will display that characteristic. It is in the heterozygous condition that it becomes clear that not all genes are created equal. Some genes are dominant, meaning they express themselves in the phenotype even when paired with a different version of the gene, while their silent partner is called recessive. Recessive genes express themselves only when paired with a similar version gene. Geneticists refer to different versions of a gene as alleles. Some dominant traits include having facial dimples, curly hair, normal vision, and dark hair. Some recessive traits include red hair, being nearsighted, and straight hair.
Most characteristics are not the result of a single gene; they are polygenic, meaning they are the result of several genes. In addition, the dominant and recessive patterns described above are usually not that simple either. Sometimes the dominant gene does not completely suppress the recessive gene; this is called incomplete dominance (Lally & Valentine-French, 2019).
Genetic Disorders
Most of the known genetic disorders are dominant gene-linked.
Recessive gene disorders, such as cystic fibrosis and sickle-cell anemia, are less common but may actually claim more lives because they are less likely to be detected as people are unaware that they are carriers of the disease.
Some genetic disorders are sex-linked; the defective gene is found on the X-chromosome. Males have only one X chromosome so are at greater risk for sex-linked disorders due to a recessive gene such as hemophilia, color-blindness, and baldness. For females to be affected by recessive genetic defects, they need to inherit the recessive gene on both X-chromosomes. But if the defective gene is dominant, females are equally at risk.
Recessive Disorders (Homozygous): The individual inherits a gene change from both parents. If the gene is inherited from just one parent, the person is a carrier and does not have the condition.
| Disorder | Description | Incidence |
| Sickle Cell Disease (SCD) | A condition in which the red blood cells in the body are shaped like a sickle (like the letter C) and affect the ability of the blood to transport oxygen. | 1 in 500 Black births
1 in 36,000 Hispanic births 1 in 2,500 babies born in Canada |
| Cystic Fibrosis (CF) | A condition that affects breathing and digestion due to thick mucus building up in the body, especially the lungs and digestive system. In CF, the mucus is thicker than normal and sticky. | 1 in 3,600 live births in Canada |
| Phenylketonuria (PKU) | A metabolic disorder in which the individual cannot metabolize phenylalanine, an amino acid. Left untreated, intellectual deficits occur. PKU is easily detected and is treated with a special diet. | 1 in 12,000 births in Canada |
| Tay Sachs Disease | Caused by an enzyme deficiency resulting in the accumulation of lipids in the nerves cells of the brain. This accumulation results in progressive damage to the cells and a decrease in cognitive and physical development. Death typically occurs by age five. | 1 in 320,000 births in the general population
1 in 30 people of Ashkenazi Jewish descent is a carrier 1 in 20 people of French-Canadian descent is a carrier |
| Albinism | When the individual lacks melanin and processes little to no pigment in the skin, hair, and eyes. Vision problems can also occur. | 1 in every 17,000 – 20,000 people in North America and Europe |
Table 2: Recessive Disorders (Homozygous) (Lally & Valentine-French, 2019).
Autosomal Dominant Disorders (Heterozygous): In order to have the disorder, the individual only needs to inherit the gene change from one parent.
| Disorder | Description | Incidence |
| Huntington’s Disease | A condition that affects the individual’s nervous system. Nerve cells become damaged, causing various parts of the brain to deteriorate. The disease affects movement, behaviour and cognition. It is fatal, and occurs at midlife. | 1 in 10,000 |
| Tourette Syndrome | A tic disorder which results in uncontrollable motor and vocal tics as well as body jerking | 1 in 250 |
| Achondroplasia | The most common form of disproportionate short stature. The individual has abnormal bone growth resulting in short stature, disproportionately short arms and legs, short fingers, a large head, and specific facial features. | 1 in 15,000-40,000 |
Table 3 : Autosomal Dominant Disorders (Heterozygous) (Lally & Valentine-French, 2019).
Sex-Linked Disorders: When the X chromosome carries the mutated gene, the disorder is referred to as an X-linked disorder. Males are more affected than females because they possess only one X chromosome without an additional X chromosome to counter the harmful gene.
| Disorder | Description | Incidence |
| Fragile X Syndrome | Occurs when the body cannot make enough of a protein it needs for the brain to grow and problems with learning and behavior can occur. Fragile X syndrome is caused from an abnormality in the X chromosome, which then breaks. If a female has a fragile X, her second X chromosome usually is healthy, but males with fragile X don’t have a second healthy X chromosome. This is why symptoms of Fragile X usually are more serious in males. | 1 in 4000 males
1 in 8000 females |
| Hemophilia | Occurs when there are problems in blood clotting causing both internal and external bleeding. Hemophilia is more common in males than females. The two most common types are hemophilia A and hemophilia B. | Hemophilia A: leas than 1 in 10,000 people in Canada
Hemophilia B: 1 in 50,000 people in Canada |
| Duchenne Muscular Dystrophy | A weakening of the muscles resulting in an inability to move, wasting away, and possible death. This form of muscular dystrophy affects males almost exclusively. | 1 in 3500 Male live births |
Table 4: Sex-Linked Disorders (Lally & Valentine-French, 2019).
Chromosomal Abnormalities: A chromosomal abnormality occurs when a child inherits too many or two few chromosomes. Some gametes do not divide evenly when they are forming. Therefore, some cells have more than 46 chromosomes. In fact, it is believed that close to half of all zygotes have an odd number of chromosomes. Most of these zygotes fail to develop and are spontaneously aborted by the mother’s body (Lally & Valentine-French, 2019, p.38).
Autosomal Chromosome Disorders: The individual inherits too many or two few chromosomes.
| Disorder | Description |
| Down Syndrome/ Trisomy 21 | Caused by an extra chromosome 21 and includes a combination of birth defects. Affected individuals have some degree of intellectual disability, characteristic facial features, often heart defects, and other health problems. The severity varies greatly among affected individuals. In Canada, approximately 1 in every 781 babies is born with Down Syndrome While the risk of having a baby with Down Syndrome increases with the mother’s age, half of babies born with Down Syndrome are born to mothers under 35 years of age. (Reference: Canadian Down Syndrome Society). |
| Trisomy 9 Mosaicism | Caused by having an extra chromosome 9 in some cells. The severity of effects relates to the proportion of cells with extra chromosomes. The effects include fetal growth restriction resulting in low birth weight and multiple anomalies, including facial, cardiac, musculoskeletal, genital, kidney, and respiratory abnormalities. |
| Trisomy 13 | Caused by an extra chromosome 13. Affected individuals have multiple birth defects and generally die in the first weeks or months of life. |
| Trisomy 18 | Caused by an extra chromosome 18 and the affected individual also has multiple birth defects and early death. |
Table 5: Autosomal Chromosomal Disorders (Trisomy 9 Mosaicism Diagnosed In Utero by Hironori Takahashi, Satoshi Hayashi, Yumiko Miura, Keiko Tsukamoto, Rika Kosaki, Yushi Itoh, and Haruhiko Sago is licensed under CC BY 3.0).


Sex-linked Chromosome Disorders: When the abnormality is on 23rd pair, the result is a sex-linked chromosomal abnormality. This happens when a person has less than or more than two sex chromosomes (Lally & Valentine-French, 2019, p. 38).
| Disorder | Description |
| Turner Syndrome (XO) | Caused when all or part of one of the X chromosomes is lost before or soon after conception due to a random event. The resulting zygote has an XO composition. Turner Syndrome affects cognitive functioning and sexual maturation in girls. Infertility and a short stature may be noted. |
| Klinefelter Syndrome (XXY) | Caused when an extra X chromosome is present in the cells of a male due to a random event. The Y chromosome stimulates the growth of male genitalia, but the additional X chromosome inhibits this development. The male can have some breast development, infertility, and low levels of testosterone. |
| XXY Syndrome | Caused when an extra Y chromosome is present in the cells of a male. There are few symptoms. They may include being taller than average, acne, and an increased risk of learning problems. The person is generally otherwise normal, including normal fertility. |
| Triple X Syndrome (XXX) | Caused when an extra X chromosome is present in the cells of a female. It may result in being taller than average, learning difficulties, decreased muscle tone, seizures, and kidney problems. |
Table 6: Sex-Linked Chromosomal Disorders (XYY Syndrome by Wikipedia is licensed under CC BY-SA 3.0; Triple X Syndrome by Wikipedia is licensed under CC BY-SA 3.0).
Triple Screening in Pregnancy: The triple screen blood test is one type of genetic screening test. It measures alpha-fetoprotein, human chorionic gonadotropin and unconjugated estriol. An abnormal test result is not a diagnosis, only an indication that the baby might be at higher risk for some birth defects. Additional testing is usually required, such as an ultrasound or amniocentesis.
Prenatal Development
Now we turn our attention to prenatal development which is divided into three periods: The germinal period, the embryonic period, and the fetal period. The following is an overview of some of the changes that take place during each period.
The Germinal Period
The germinal period (about 14 days in length) lasts from conception to implantation of the fertilized egg in the lining of the uterus. At ejaculation millions of sperm are released into the vagina, but only a few reach the egg and typically only one fertilizes the egg. Once a single sperm has entered the wall of the egg, the wall becomes hard and prevents other sperm from entering. After the sperm has entered the egg, the tail of the sperm breaks off and the head of the sperm, containing the genetic information from the father, unites with the nucleus of the egg. It is typically fertilized in the top section of the fallopian tube and continues its journey to the uterus. As a result, a new cell is formed. This cell, containing the combined genetic information from both parents, is referred to as a zygote.

Image: Sperm and ovum at conception. (Image is in the public domain)
During this time, the organism begins cell division through mitosis. After five days of mitosis there are 100 cells, which is now called a blastocyst. The blastocyst consists of both an inner and outer group of cells. The inner group of cells, or embryonic disk will become the embryo, while the outer group of cells, or trophoblast, becomes the support system which nourishes the developing organism. This stage ends when the blastocyst fully implants into the uterine wall (U.S. National Library of Medicine, 2015, as cited in Paris et al., 2021).
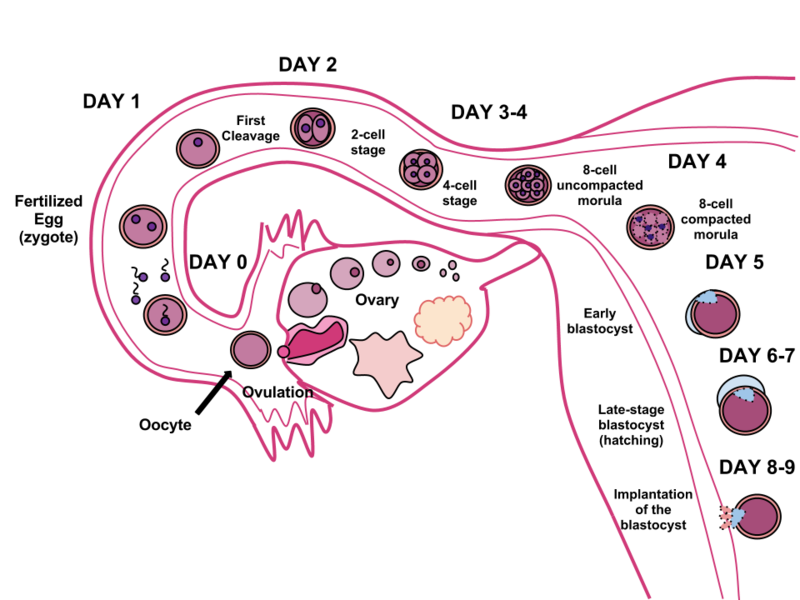
Mitosis is a fragile process and fewer than one half of all zygotes survive beyond the first two weeks (Hall, 2004). Some of the reasons for this include: The egg and sperm do not join properly, thus their genetic material does not combine, there is too little or damaged genetic material, the zygote does not replicate, or the blastocyst does not implant into the uterine wall. The image above illustrates the journey of the ova from its release to its fertilization, cell duplication, and implantation into the uterine lining (Lally & Valentine-French, 2019,p. 42-43).
The Embryonic Period
Starting the third week, the blastocyst has implanted in the uterine wall. Upon implantation this multi-cellular organism is called an embryo. Now blood vessels grow forming the placenta. The placenta is a structure connected to the uterus that provides nourishment and oxygen from the mother to the developing embryo via the umbilical cord.
During this period, cells continue to differentiate. Growth during prenatal development occurs in two major directions: from head to tail called cephalocaudal development and from the midline outward referred to as proximodistal development. This means that those structures nearest the head develop before those nearest the feet and those structures nearest the torso develop before those away from the center of the body (such as hands and fingers). You will see that this pattern continues after birth.
The head develops in the fourth week and the precursor to the heart begins to pulse. In the early stages of the embryonic period, gills and a tail are apparent. However, by the end of this stage they disappear and the organism takes on a more human appearance.

Image: A human embryo. (Image by Anatomist90 is licensed under CC BY-SA 3.0)
About 20 percent of organisms fail during the embryonic period, usually due to gross chromosomal abnormalities, often before the mother even knows that she is pregnant. It is during this stage that the major structures of the body are taking form, making the embryonic period the time when the organism is most vulnerable to the greatest amount of damage if exposed to harmful substances. Prospective mothers are not often aware of the risks they introduce to the developing embryo during this time. The embryo is approximately 1 inch in length and weighs about 4 grams at the end of eight weeks. The embryo can move and respond to touch at this time. (Lally & Valentine-French, 2019, p. 43).
The Fetal Period
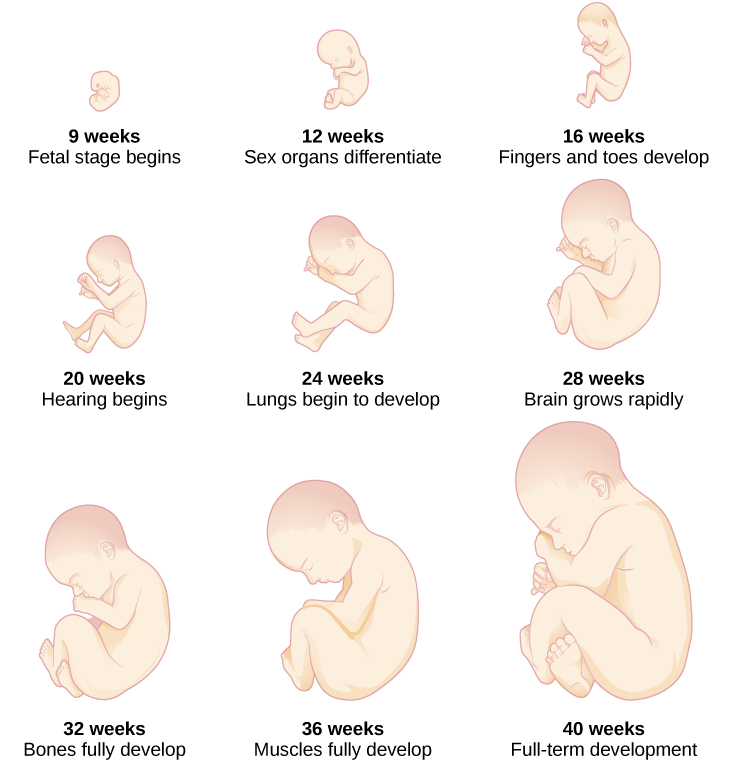
From the ninth week until birth (which is forty weeks for a full-term pregnancy), the organism is referred to as a fetus. During this stage, the major structures are continuing to develop. By the third month, the fetus has all its body parts including external genitalia. The fetus is about 3 inches long and weighs about 28 grams. In the following weeks, the fetus will develop hair, nails, teeth and the excretory and digestive systems will continue to develop.

Image: A human fetus. (Image by lunar caustic is licensed under CC BY-SA 2.0)
During the 4th – 6th months, the eyes become more sensitive to light and hearing develops. The respiratory system continues to develop, and reflexes such as sucking, swallowing and hiccupping, develop during the 5th month. Cycles of sleep and wakefulness are present at this time as well. The first chance of survival outside the womb, known as the age of viability is reached at about 24 weeks (Morgan, Goldenberg, & Schulkin, 2008, as cited in Paris et al., 2021). The majority of the neurons in the brain have developed by 24 weeks, although they are still rudimentary, and the glial or nurse cells that support neurons continue to grow. At 24 weeks the fetus can feel pain (Royal College of Obstetricians and Gynecologists, 1997, as cited in Paris et al., 2021).
Between the 7th – 9th months, the fetus is primarily preparing for birth. It is exercising its muscles and its lungs begin to expand and contract. The fetus gains about 5 pounds and 7 inches during this last trimester of pregnancy, and during the 8th month a layer of fat develops under the skin. This layer of fat serves as insulation and helps the baby regulate body temperature after birth.
At around 36 weeks the fetus is almost ready for birth. It weighs about 6 pounds and is about 18.5 inches long. By week 37 all of the fetus’s organ systems are developed enough that it could survive outside the mother’s uterus without many of the risks associated with premature birth. The fetus continues to gain weight and grow in length until approximately 40 weeks. By then the fetus has very little room to move around and birth becomes imminent. The progression through the stages is shown in the following image (Lally & Valentine-French, 2019, p. 44).
Monozygotic and Dizygotic Twins
Monozygotic or identical twins occur when a fertilized egg splits apart in the first two weeks of development. The result is the creation of two separate identical offspring. That is, they possess the same genotype and often the same phenotype. About one-third of twins are monozygotic twins.
Sometimes, however, two eggs or ova are released and fertilized by two separate
sperm. The result is dizygotic or fraternal twins. These two individuals share the amount of genetic material as would any two children from the same mother and father. In other words, they possess a different genotype and phenotype.
Older mothers are more likely to have dizygotic twins than are younger mothers, and couples who use fertility drugs are also more likely to give birth to twins (Lally & Valentine-French, 2019, p. 36) .
Teratogens
Good prenatal care is essential to protect against maternal and fetal/infant mortality and birth complications. The embryo and fetus are most at risk for some of the most severe problems during the first three months of development. Unfortunately, this is a time at which many mothers are unaware that they are pregnant. Today, we know many of the factors that can jeopardize the health of the developing child. Teratogens are environmental factors that can contribute to birth defects, and include some maternal diseases, pollutants, drugs and alcohol. The study of these factors that contribute to birth defects is called teratology.
There are four categories of teratogens:
- Physical teratogens: These could be saunas, hot tubs, or infections that raise a pregnant woman’s body temperature to 102 degrees Fahrenheit or higher. This is associated with neural tube defects, spontaneous abortions, and various cardiovascular abnormalities.
- Metabolic conditions affecting pregnant females: Metabolic conditions are abnormalities in the chemical process of producing energy from food, and thereby affect the development and function of the body. If a pregnant woman is malnourished, then her fetus likely lacks the nutrients essential for its development. These include: malnutrition, diabetes, and thyroid disorders.
- Infections: Different maternal infections, including rubella virus, herpes simplex virus, and syphilis can cause congenital abnormalities in fetuses.
- Drugs and chemicals: When pregnant females ingest or absorb these, they may cause a variety of different effects based on specific agent, amount of exposure, and timing. This category includes: radiation, heavy metals (including lead), insecticides and herbicides, prescription and over the counter drugs, illicit and recreational drugs, alcohol, cigarettes, nicotine, caffeine, and even some vitamins (Tantibanchachai, 2014).
While there are many, many potential teratogens, the following tables look at the effects of some different types of teratogens. The risks of exposure vary based on lifestyle and health. The effects may vary greatly depending on the factors mentioned previously. Protection and prevention will vary based on the method of exposure. The following table has been adapted from Lumen Learning (n.d.).
| Teratogen | Potential Effects |
| Caffeine | Moderate amounts of caffeine (200 mg or around 12 ounces of coffee) appear to be safe during pregnancy. Some studies have shown a link between higher amounts of caffeine and miscarriage and preterm birth. (Office of Women’s Health, as cited by Lumen Learning, n.d.) |
| Tobacco | Tobacco use has been associated with low birth weight, placenta previa, preterm delivery, fetal growth restriction, sudden infant death syndrome, cleft lip or palate, and later health problems (such as high blood pressure and diabetes) (Lumen Learning, n.d.) |
| Alcohol | There is no safe amount of alcohol a woman can drink while pregnant. Alcohol can slow down the baby’s growth, affect the baby’s brain, and cause birth defects, and may results in fetal alcohol spectrum disorder (FASD). The effects can be mild to severe. Children born with a severe form of FASD can have abnormal facial features, severe learning disabilities, behavioral problems, and other problems. (Office of Women’s Health, as cited by Lumen Learning, n.d.) |
| Cocaine | Cocaine use has connected with low birth weight, stillbirths, spontaneous abortion, placental abruption, premature birth, miscarriage, and neonatal abstinence syndrome (fetal addiction leads the newborn to experiences withdrawal) (Office of Women’s Health, as cited by Lumen Learning, n.d.) |
| Marijuana | No amount of marijuana has been proven safe to use during pregnancy. Heavy use has been associated with brain damage, premature birth, and stillbirth (Lumen Learning, n.d.) |
| Heroin | Using heroin during pregnancy can cause birth defects, placental abruption, premature birth, low birthweight, neonatal abstinence syndrome, still birth, and sudden infant death syndrome (March of Dimes, as cited in Lumen Learning, n.d.). |
| Over-the-Counter (OTC) medication | Some OTC medications are safe to use during pregnancy and others may cause health problems during pregnancy. Pregnant women should consult their health care provider before using OTC medications (March of Dimes, as cited in Lumen Learning, n.d.). |
| Prescription drugs | Some prescription drugs can cause birth defects that change the shape or function of one or more parts of the body that can affect overall health. Pregnant women should consult their health care provider before discontinuing or starting new medications (March of Dimes, as cited in Lumen Learning, n.d.). |
| Herbal or dietary supplements | Except for some vitamins, little is known about using herbal or dietary supplements while pregnant. Most often there are no good studies to show if the herb can cause harm to you or your baby. Also, some herbs that are safe when used in small amounts as food might be harmful when used in large amounts as medicines (Lumen Learning, n.d.) |
Table 7 – Drugs as Teratogens (Paris et al., 2021)
| Teratogen | Potential Effects |
| Lead | Exposure to high levels of lead before and during pregnancy can lead to high blood pressure, problems with fetal brain and nervous system development, premature birth, low birthweight, and miscarriage.Prescription drugs, over-the-counter drugs, supplements and herbal products (n.d.). Retrieved from: https://www.marchofdimes.org/pregnancy/prescription-drugs-over-the-counter-drugs-supplements-and-herbal- products.aspx[ |
| Mercury | Exposure to mercury in the womb can cause brain damage and hearing and vision problems.Prescription drugs, over-the-counter drugs, supplements and herbal products (n.d.). Retrieved from: https://www.marchofdimes.org/pregnancy/prescription-drugs-over-the-counter-drugs-supplements-and-herbal- products.aspx[ |
| Radiation | Exposure to radiation during pregnancy (especially between 2 and 18 weeks of pregnancy) can slow growth, cause birth defects, affect brain development, cause cancer, and cause miscarriage.Prescription drugs, over-the-counter drugs, supplements and herbal products (n.d.). Retrieved from: https://www.marchofdimes.org/pregnancy/prescription-drugs-over-the-counter-drugs-supplements-and-herbal- products.aspx[ |
| Solvents | These chemicals include degreasers, paint thinners, stain and varnish removers, paints, and more Maternal inhalation of solvents can cause fetal exposure than may cause miscarriage, slow fetal growth, premature birth, and birth defects.Prescription drugs, over-the-counter drugs, supplements and herbal products (n.d.). Retrieved from: https://www.marchofdimes.org/pregnancy/prescription-drugs-over-the-counter-drugs-supplements-and-herbal- products.aspx[ |
| Radon | Radon is a radioactive gas naturally found in the environment when uranium in soil and rock breaks down. Radon is odorlous, invisible and tasteless. Research in this area is limited, but one unreplicated research study in 2016 concluded there is an association between residential radon levels and the occurrence of cleft lip and cystic hygroma (a fluid-filled sac that results from a blockage in the lymphatic system). (Langlois, P. H., Lee, M., Lupo, P. J., Rahbar, M. H., & Cortez, R. K. (2016). Residential radon and birth defects: A population-based assessment. Birth defects research. Part A, Clinical and molecular teratology, 106(1), 5–15. https://doi.org/10.1002/bdra.23369) |
Table 2.8 – Environmental Teratogens (Paris et al., 2021)
| Teratogen | Potential Effects |
| Rubella | Congenital infection (becoming infected while in the womb) can damage the development of the eyes, ears, heart, and brain and result in deafness.Chapter 3: Prenatal Development – Environmental Risks references Psyc 200 Lifespan Psychology by Laura Overstreet, which is licensed under CC BY 4.0[ |
| Zika | Congenital infection can cause microcephaly and other severe brain abnormalities.Protocols on prenatal care for pregnant women with Zika infection and children with microcephaly: nutritional approach by Rachel de Sá Barreto Luna Callou Cruz, Malaquias Batista Filho, Maria de Fátima Costa Caminha, and Edvaldo da Silva Souza is licensed under CC BY 4.0[ |
| Varicella (chicken pox) | Congenital infection can cause a severe form of the infection affecting the eyes, limbs, skin, and central nervous system.Congenital Varicella syndrome by WikiDoc is licensed under CC BY-SA 3.0[ |
| Sexually transmitted infections | Infections such as HIV, gonorrhea, syphilis, and chlamydia can be passed from the mother during pregnancy and/or delivery.Chapter 3: Prenatal Development – Environmental Risks references Psyc 200 Lifespan Psychology by Laura Overstreet, which is licensed under CC BY 4.0[ |
| Listeria | Pregnant women are more susceptible to this food-borne illness. Congenital infection can cause miscarriage, stillbirth, premature labor, and neonatal sepsis.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2860824/[ |
Table 9: Maternal Infections as Teratogens (as cited in Paris et al., 2021)
| Teratogen | Potential Effects |
| Toxoplamosis | This parasite can be passed through cat feces and undercooked meat (especially pork, lamb, or deer meat). If the fetus is infected it can cause miscarriage, stillbirth, hydrocephalus, macro or microcephalus, vision issues, and damage to the nervous system.Prescription drugs, over-the-counter drugs, supplements and herbal products (n.d.). Retrieved from: https://www.marchofdimes.org/pregnancy/prescription-drugs-over-the-counter-drugs-supplements-and-herbal- products.aspx[ |
| Lymphocytic choriomeningitis | This virus carried by rodents including mice, hamsters, and guinea pigs. If an infected mother passes it to her fetus it can cause issues with brain development, long-term neurological and/or visual impairment, and higher mortality rates after birth.Prescription drugs, over-the-counter drugs, supplements and herbal products (n.d.). Retrieved from: https://www.marchofdimes.org/pregnancy/prescription-drugs-over-the-counter-drugs-supplements-and-herbal- products.aspx[ |
Table 10: Teratogens from Animals/Pets (as cited in Paris et al., 2021)
Factors influencing prenatal risks: There are several considerations in determining the type and amount of damage that might result from exposure to a particular teratogen (Berger, 2005, as cited in Paris et al., 2021). These include:
- The timing of the exposure: Structures in the body are vulnerable to the most severe damage when they are forming. If a substance is introduced during a particular structure’s critical period (time of development), the damage to that structure may be greater. For example, the ears and arms reach their critical periods at about 6 weeks after conception. If a mother exposes the embryo to certain substances during this period, the arms and ears may be malformed. (see figure below)
- The amount of exposure: Some substances are not harmful unless the amounts reach a certain level. The critical level depends in part on the size and metabolism of the mother.
- The number of teratogens: Fetuses exposed to multiple teratogens typically have more problems than those exposed to only one.
- Genetics: Genetic makeup also plays a role on the impact a particular teratogen might have on the child. This is suggested by fraternal twins exposed to the same prenatal environment, but they do not experience the same teratogenic effects. The genetic makeup of the mother can also have an effect; some mothers may be more resistant to teratogenic effects than others.
- Being male or female: Males are more likely to experience damage due to teratogens than are females. It is believed that the Y chromosome, which contains fewer genes than the X, may have an impact (Lally & Valentine-French, 2019, p. 46/47).
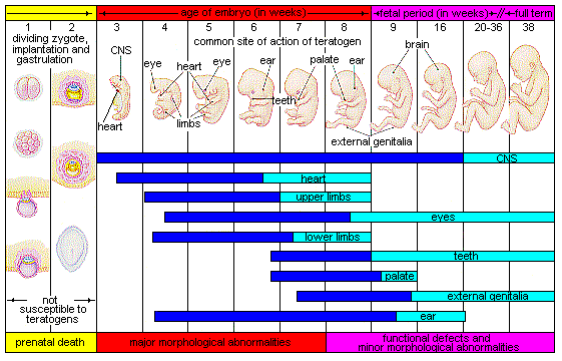
Figure: The development of an embryo into a fetus. (Image by Laura Overstreet is licensed under CC BY-NC-SA 3.0)
Other factors that can affect pregnancy
Maternal Factors
There are additional factors that affect the outcome of pregnancy for both mother and child. Let’s look at these next.
Mothers over 35
Most women over 35 who become pregnant are in good health and have healthy pregnancies. However, according to the March of Dimes (2016d, as cited in as cited in Paris et al., 2021), women over age 35 are more likely to have an increased risk of:
- Fertility problems
- High blood pressure
- Diabetes
- Miscarriages
- Placenta Previa
- Cesarean section
- Premature birth
- Stillbirth
- A baby with a genetic disorder or other birth defects
Because a woman is born with all her eggs, environmental teratogens can affect the quality of the eggs as women get older. Also, a woman’s reproductive system ages which can adversely affect the pregnancy. Some women over 35 choose special prenatal screening tests, such as a maternal blood screening, to determine if there are any health risks for the baby.
Although there are medical concerns associated with having a child later in life, there are also many positive consequences to being a more mature parent. Older parents are more confident, less stressed, and typically married, providing family stability. Their children perform better on math and reading tests, and they are less prone to injuries or emotional troubles (Albert, 2013, as cited in as cited in Paris et al., 2021). Women who delay pregnancy either by choice or because of challenges with conceiving are often better educated and have healthier lifestyles. According to Gregory (2007, as cited in as cited in Paris et al., 2021), older women are more stable, demonstrate a stronger family focus, possess greater self-confidence, and have more money. Having a child later in one’s career equals overall higher wages. In fact, for every year a woman delays motherhood, she makes 9% more in lifetime earnings. Lastly, women who delay having children actually live longer.
Teenage Pregnancy
A teenage mother is at a greater risk for having pregnancy complications including anemia, and high blood pressure.
These risks are even greater for those under age 15. Infants born to teenage mothers have a higher risk for being premature and having low birthweight or other serious health problems. Premature and low birthweight babies may have organs that are not fully developed which can result in breathing problems, bleeding in the brain, vision loss, serious intestinal problems, and higher likelihood of dying. Reasons for these health issues include that teenagers are the least likely of all age groups to get early and regular prenatal care and they may engage in negative behaviours including eating unhealthy food, smoking, drinking alcohol, and taking drugs.
Gestational Diabetes
Gestational diabetes can occur if the body cannot produce enough insulin to adapt to the effects of a growing fetus and changing hormone levels. The cells become resistant to the action of insulin and, in turn, the pancreas cannot secrete enough insulin to counterbalance the effect of these hormones.
In Canada, between 3% and 20% of pregnant women develop gestational diabetes, depending on their risk factors. While the rate for all pregnancies is roughly 2%-4%, the rate in First Nations women has been reported to be between 8% and 18% (Diabetes Canada, 2022). Research by Dyck et al. (2002, as cited in First Nations Centre, National Aboriginal Health Organization, 2009) concluded that First Nations ancestry is an independent risk factor; that is, even when a woman has none of the other risk factors for developing gestational diabetes, if she is of First Nations ancestry, she is more likely to develop gestational diabetes. The researchers concluded that the reasons for this were unclear.
Most pregnant women have their glucose level tested between 24 to 28 weeks of pregnancy. Gestational diabetes usually goes away after the mother gives birth, but it might indicate a risk for developing diabetes later in life. If untreated, gestational diabetes can cause premature birth, stillbirth, the baby having breathing problems at birth, jaundice, or low blood sugar. Babies born to mothers with gestational diabetes can also be considerably heavier (more than 9 pounds) making the labor and birth process more difficult. For expectant mothers, untreated gestational diabetes can cause preeclampsia (high blood pressure and signs that the liver and kidneys may not be working properly) discussed later in the chapter.
Risk factors for gestational diabetes include age (being over age 25), being overweight or gaining too much weight during pregnancy, family history of diabetes, having had gestational diabetes with a prior pregnancy, and race and ethnicity. In addition to women with First Nation ancestry, African-American, Native American, Hispanic, Asian, or Pacific Islander have a higher risk. Eating healthy, exercising regularly and maintaining a healthy weight during pregnancy can reduce the chance of developing gestational diabetes. If these actions are unsuccessful at controlling blood sugar levels, insulin may be required. Women who already have diabetes and become pregnant need to attend all their prenatal care visits, and follow the same advice as those for women with gestational diabetes as the risk of preeclampsia, premature birth, birth defects, and stillbirth are the same.
High Blood Pressure (Hypertension)
Hypertension is a condition in which the pressure against the wall of the arteries becomes too high. There are two types of high blood pressure during pregnancy, gestational and chronic. Gestational hypertension only occurs during pregnancy and goes away after birth. Chronic high blood pressure refers to women who already had hypertension before the pregnancy or to those who developed it during pregnancy and it did not go away after birth.
According to the March of Dimes (2015, as cited in Paris et al., 2021), about 8 in every 100 pregnant women have high blood pressure. High blood pressure during pregnancy can cause premature birth and low birth weight (under five and a half pounds), placental abruption, and mothers can develop preeclampsia.
Rh Disease
Rh is a protein found in the blood. Most people are Rh positive, meaning they have this protein. Some people are Rh negative, meaning this protein is absent. Mothers who are Rh negative are at risk of having a baby with a form of anemia called Rh disease (March of Dimes, 2009). A father who is Rh-positive and mother who is Rh-negative can conceive a baby who is Rh-positive. Some of the fetus’s blood cells may get into the mother’s bloodstream and her immune system is unable to recognize the Rh factor.
The immune system starts to produce antibodies to fight off what it thinks is a foreign invader. Once her body produces immunity, the antibodies can cross the placenta and start to destroy the red blood cells of the developing fetus. As this process takes time (longer than 9 months), often the first Rh positive baby is not harmed, but as the mother’s body will continue to produce antibodies to the Rh factor across her lifetime, subsequent pregnancies can pose greater risk for an Rh positive baby. When there is Rh incompatibility (Rh negative woman conceives an Rh positive baby), RhoGAM, a manufactured antibody, is given to the pregnant woman at 28 weeks and again after delivery. This prevents the mother from developing the antibodies that would attack the baby’s blood cells in the event her blood crosses the placenta. In the newborn, Rh disease can lead to jaundice, anemia, heart failure, brain damage and death.
Stress
Feeling stressed is common during pregnancy, but high levels of stress can cause complications including having a premature baby or a low-birthweight baby. Babies born early or too small are at an increased risk for health problems. Stress-related hormones may cause these complications by affecting a woman’s immune systems resulting in an infection and premature birth. Additionally, some women deal with stress by smoking, drinking alcohol, or taking drugs, which can lead to problems in the pregnancy. High levels of stress in pregnancy have also been correlated with problems in the baby’s brain development and immune system functioning, as well as childhood problems such as trouble paying attention and being afraid (March of Dimes, 2012, as cited in Paris et al., 2021).
Nutrition
As the fetus develops in the womb, this growth uses a lot of resources from the mother, and having adequate nutrition and access to the necessary foods, vitamins, etc. that support prenatal growth is key. The Canada Prenatal Nutrition Program (CPNP) provides information and supports the health and well-being of pregnant people, providing programs and access to inclusive supports along the way (Government of Canada, 2021).
Depression
Depression is a significant medical condition in which feelings of sadness, worthlessness, guilt, and fatigue interfere with one’s daily functioning. According to the Mayo Clinic, about 7% of women experience depression during pregnancy (Mayo Clinic, 2022).
Women who have experienced depression previously are more likely to have depression during pregnancy. Consequences of depression include the baby being born premature, having a low birth weight, being more irritable, less active, less attentive, and having fewer facial expressions.
About 13% of pregnant women take an antidepressant during pregnancy. It is important that women taking antidepressants during pregnancy discuss the medication with a health care provider as some medications can cause harm to the developing organism.
Experiences of Indigenous Women, BIPOC women
An extensive literature review conducted in 2016 concluded that availability of healthcare resources, healthcare services’ consideration of socio-economic or lifestyle barriers to health, and the impact of colonization on interactions with healthcare providers were main factors that impacted Indigenous women’s maternal health experiences. Medical evacuation was often due to limited maternity care options available in remote communities, and was associated with emotional, physical, and financial stress. The review highlighted the importance of consistent health policies and practices for maternal health in Canada and providing culturally safe and patient-centered maternity healthcare services within indigenous communities (Kolahdooz, Launier, Nader, Yi, Baker, McHugh, Vallianatos & Sharma, 2016).
Kenhteke Midwives on the Tyendinaga Mohawk Territory in Canada is an example of culturally appropriate maternal and newborn care that “sustains our way of life by birthing our children in the hands of our own people, on our land, using our language, traditions, culture and traditional medicines” (Kenhteke Midwives, 2017).
To learn more about BIPOC women and pregnancy: https://www.consciouspregnancy.ca/bipoc
Paternal Factors
Male fertility is also affected by age. The quality of semen starts to decline after the age of 35. Sperm motility also declines with age. Genetic defects in sperm increase with age. These defects have been associated with: decreased fertility, increased risk of miscarriage, increase risk of some birth defects and increase risk of stillbirth (Gurevich, 2020).
Paternal Impact
The age of fathers at the time of conception is also an important factor in health risks for children. According to Nippoldt (2015, as cited in Paris et al., 2021), offspring of men over 40 face an increased risk of miscarriages, autism, birth defects, achondroplasia (bone growth disorder) and schizophrenia. These increased health risks are thought to be due to accumulated chromosomal aberrations and mutations during the maturation of sperm cells in older men (Bray, Gunnell, & Smith, 2006, as cited in Paris et al., 2021). However, like older women, the overall risks are small.

In addition, men are more likely than women to work in occupations where hazardous chemicals, many of which have teratogenic effects or may cause genetic mutations, are used (Cordier, 2008, as cited in Paris et al., 2021). These may include petrochemicals, lead, and pesticides that can cause abnormal sperm and lead to miscarriages or diseases. Men are also more likely to be a source of second hand smoke for their developing offspring. As noted earlier, smoking by either the mother or around the mother can hinder prenatal development (Lally & Valentine-French, 2019. p.52).
Prenatal Assessment
A number of assessments are suggested to women as part of their routine prenatal care to find conditions that may increase the risk of complications for the mother and fetus (Eisenberg, Murkoff, & Hathaway, 1996, as cited in Paris et al., 2021). These can include blood and urine analyses and screening and diagnostic tests for birth defects.

Ultrasound is one of the main screening tests done in combination with blood tests. The ultrasound is a test in which sound waves are used to examine the fetus. There are two general types. Transvaginal ultrasounds are used in early pregnancy, while transabdominal ultrasounds are more common and used after 10 weeks of pregnancy (typically, 16 to 20 weeks).
Ultrasounds are used to check the fetus for defects or problems. It can also find out the age of the fetus, location of the placenta, fetal position, movement, breathing and heart rate, amount of amniotic fluid in the uterus, and number of fetuses. Most women have at least one ultrasound during pregnancy, but if problems are noted, additional ultrasounds may be recommended.
When diagnosis of a birth defect is necessary, ultrasounds help guide the more invasive diagnostic tests of amniocentesis and chorionic villus sampling. Amniocentesis is a procedure in which a needle is used to withdraw a small amount of amniotic fluid and cells from the sac surrounding the fetus and later tested.
Chorionic Villus Sampling is a procedure in which a small sample of cells is taken from the placenta and tested. Both amniocentesis and chorionic villus sampling have a risk of miscarriage, and consequently they are not done routinely (Lally & Valentine-French, 2019).
Side Effects of Pregnancy
There are a number of common side effects of pregnancy. Not everyone experiences all of these, nor to the same degree. In most cases, these side effects will not harm the developing fetus, but this is not to say that they are not potentially very uncomfortable for the mother. These side effects include nausea (particularly during the first 3-4 months of pregnancy as a result of higher levels of estrogen in the system), heartburn, gas, hemorrhoids, backache, leg cramps, insomnia, constipation, shortness of breath or varicose veins (as a result of carrying a heavy load on the abdomen).
But there are also serious complications of pregnancy which can pose health risks to mother and child and that often require hospitalization.
Hyperemesis gravidarum is characterized by severe nausea, vomiting, weight loss, and possibly dehydration. Signs and symptoms may also include vomiting many times a day and feeling faint. The exact causes of hyperemesis gravidarum are unknown. Risk factors include the first pregnancy, multiple pregnancy, obesity, prior or family history of HG, trophoblastic disorder, and a history of eating disorders. Treatment includes drinking fluids and a bland diet. Medication, intravenous fluids, and hospitalization may be required. Hyperemesis gravidarum is estimated to affect 0.3–2.0% of pregnant women. Those affected have a low risk of miscarriage but a higher risk of premature birth.
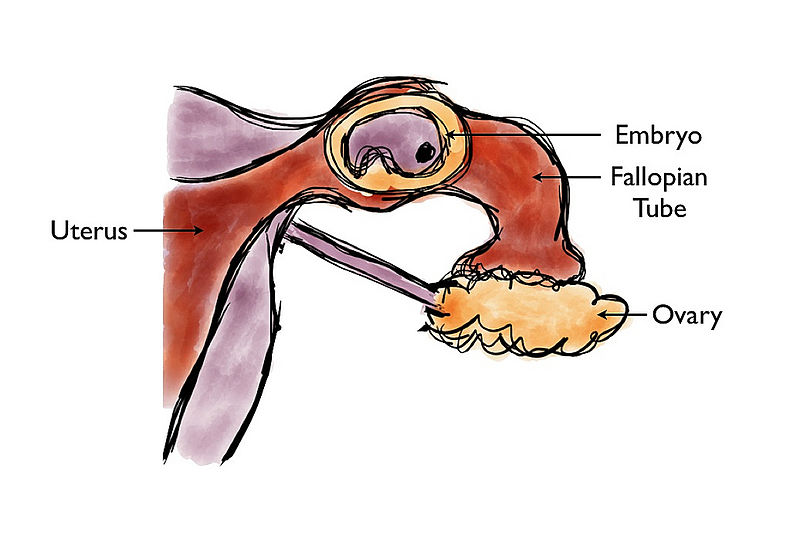
Ectopic Pregnancy occurs when the zygote becomes attached to the fallopian tube before reaching the uterus. The rate of ectopic pregnancy is about 2% in the general population (Canadian Medical Association Journal, 2005).
This number has been increasing because of the higher rates of pelvic inflammatory disease and Chlamydia (Carroll, 2007, as cited in Paris et al., 2021). Abdominal pain, vaginal bleeding, nausea and fainting are symptoms of ectopic pregnancy.
The Society of Obstetricians and Gynaecologists of Canada estimates that 15 to 20% of pregnancies end in a miscarriage. In many cases, a miscarriage is due to chromosomal abnormalities in the developing fetus, and this typically happens before the 12th week of pregnancy. Cramping and bleeding result and normal periods return after several months. Some women are more likely to have repeated miscarriages due to chromosomal, amniotic, or hormonal problems, but miscarriage can also be a result of defective sperm (Carrell et. al., 2003, as cited in Paris et al., 2021).
Preeclampsia, also known as Toxemia, is characterized by a sharp rise in blood pressure, a leakage of protein into the urine as a result of kidney problems, and swelling of the hands, feet, and face during the third trimester of pregnancy. Preeclampsia is the most common complication of pregnancy. When preeclampsia causes seizures, the condition is known as eclampsia. Preeclampsia is also a leading cause of fetal complications, which include low birth weight, premature birth, and stillbirth. Treatment is typically bed rest and sometimes medication. If this treatment is ineffective, labor may be induced.
Maternal Mortality: According to to the World Health Organization (2017), approximately 800 women around the world died each day from preventable causes related to pregnancy and childbirth. Rates are highest in Sub-Saharan Africa and South Asia, although there has been a substantial decrease in these rates. The campaign to make childbirth safe for everyone has led to the development of clinics accessible to those living in more isolated areas and training more midwives to assist in childbirth (as cited in Lally & Valentine-French, 2019, p. 58).
Childbirth
After around 266 days of developing inside the womb (for a full-term pregnancy), comes the arduous process of childbirth. For many reasons, each pregnancy and delivery is unique and influenced by social and cultural factors as well as personal choices made about preparing for childbirth. Let’s begin by exploring some of the approaches to childbirth.
Preparing for Childbirth
Prepared childbirth refers to being not only in good physical condition to help provide a healthy environment for the baby to develop, but also helping individuals to prepare to accept their new roles as parents. Additionally, parents can receive information and training that will assist them in delivery and life with the baby. The more future parents can learn about childbirth and the newborn, the better prepared they will be for the adjustment they must make to a new life.
Approaches to Childbirth
Support for Culturally Safe Indigenous Birth
Children born into their home community are more likely to develop a clear sense of identity, which helps to promote resilience and build strong community bonds. However, most Indigenous women are forced to travel to urban centres to give birth in settings that may not feel culturally secure. Care providers and administrators need to value and incorporate birth traditions, rituals, and ceremonies, provide different options for safe maternity care outside of major centres, and increase the number of Indigenous maternity care providers (e.g., midwives, doulas, birth workers).
Care providers may be well-meaning in their intentions to care for the Indigenous mother and her infant based on their professional training, but this has also resulted in birth being medicalized in Western ways with subsequent loss of traditional birth practices, ceremonies, and rituals for Indigenous families (National Aboriginal Council of Midwives, 2016, as cited in Exner-Pirot, Norbye and Butler, 2018). To offer quality maternity care to Indigenous mothers and their families, providers should work towards practicing cultural safety. Cultural safety addresses inequities arising from sociocultural factors and power differentials between service providers and those they care for; clinical practice without cultural safety contributes to the continued oppression of Indigenous peoples (Roy, 2014, as cited in Exner-Pirot, Norbye and Butler, 2018). Learning about different peoples and cultures is a key component of gaining cultural competence for care providers (Kirmayer, 2012; Tervalon & Murray-García, 1998, as cited in Exner-Pirot, Norbye and Butler, 2018). Therefore, increasing care provider understanding about traditional maternal and newborn Indigenous birthing practices and ceremonies is essential to promote cultural security for childbearing women (Exner-Pirot, Norbye and Butler, 2018).
Indigenous Perspective
Once the baby is born there is a ceremony performed that will connect the baby to mother earth (connection to the land and all creation). To learn more about Indigenous ceremonies and traditions relating to birth, read CBC’s article “Why Indigenous women are bringing ‘the first ceremony’ — birth — back to their communities” https://www.cbc.ca/radio/unreserved/indigenous-birthing-practices-1.6687501
Want to learn more about childbirth in general? For a more in depth look, check out Lumen Learning’s resource describing this in more detail: https://courses.lumenlearning.com/wm-lifespandevelopment/chapter/childbirth/
Next, we’ll talk about how a baby’s development, and potential genetic, physical, and environmental concerns are identified.
The Newborn

Assessing the Newborn
The Apgar assessment is conducted one minute and five minutes after birth. This is a very quick way to assess the newborn’s overall condition. Five measures are assessed: Heart rate, respiration, muscle tone (assessed by touching the baby’s palm), reflex response (the Babinski reflex is tested), and colour. A score of 0 to 2 is given on each feature examined. An Apgar of 5 or less is cause for concern. The second Apgar should indicate improvement with a higher score (Lally & Valentine-French, 2019, p. 63).
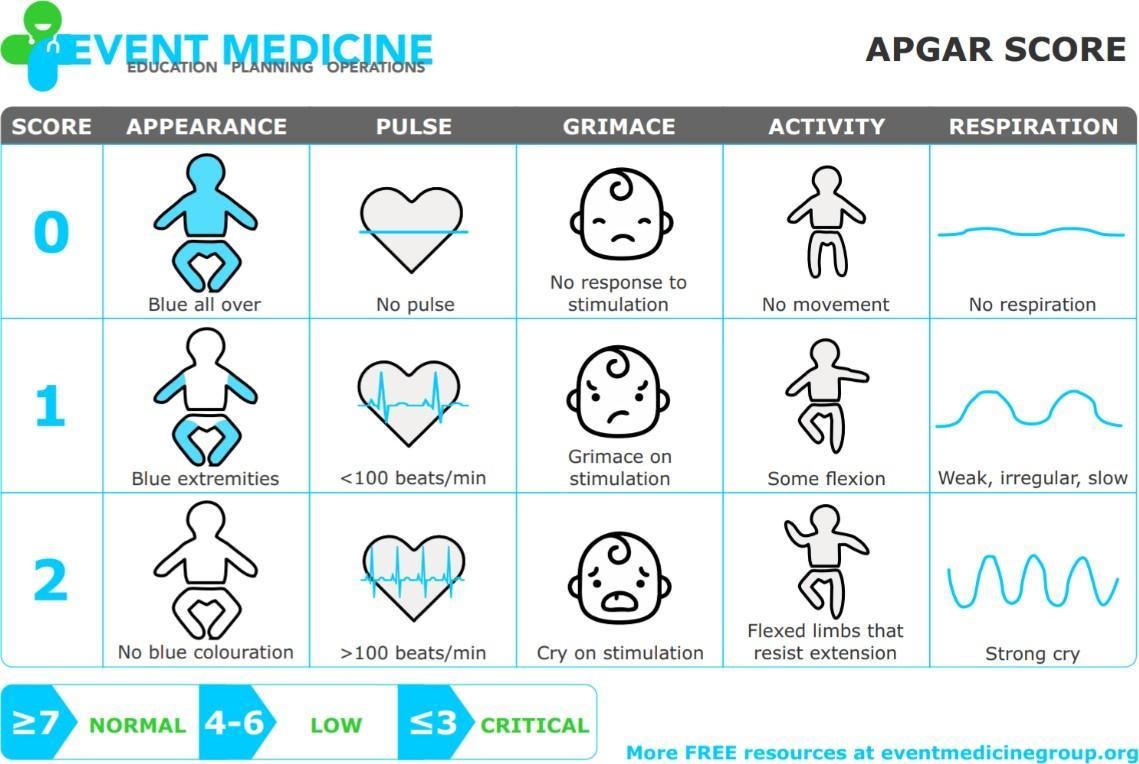
Image: The Apgar assessment. (Image by Event Medicine Group)
Another way to assess the condition of the newborn is the Neonatal Behavioral Assessment Scale (NBAS). The baby’s motor development, muscle tone, and stress response are assessed. This tool has been used around the world to further assess the newborn, especially those with low Apgar scores, and to make comparisons of infants in different cultures (Brazelton & Nugent, 1995, as cited in Paris et al., 2021).
Newborns are also routinely screened for different conditions. Within the first 24 to 48 hours after birth, babies born in hospitals undergo a simple heel stick and a few drops of blood are collected on a special paper card. Providers test those dried blood spots for a variety of different congenital disorders, or conditions that are present when the baby is born.

In Ontario all newborns in hospital and community settings have a universal hearing screening administered as part of the Infant Hearing Program. This screening identifies infants who should have more in-depth testing for hearing loss as early as possible.
Most babies will pass the newborn hearing screening which means their hearing is fine at this time (Government of Ontario, 2021).
Complications with the Newborn
Anoxia
Anoxia is a temporary lack of oxygen to the brain. Difficulty during delivery may lead to anoxia which can result in brain damage or in severe cases, death. Babies who suffer both low birth weight and anoxia are more likely to suffer learning disabilities later in life as well.
Low Birth Weight
A child is considered low birth weight if they weigh less than 2500 grams (5.5lbs). In 2017, 6.5% of babies born in Canada weighed less than 2500 grams. There are regional differences in this statistic. For example, in the Northwest Territories, 5.9% of babies were low birth weight. Ontario was slightly above the national figure at 6.7%. In Nunavut, 7.8% of babies were low birth weight (Statistics Canada, 2018).
A low birth weight baby has difficulty maintaining adequate body temperature because it lacks the fat that would otherwise provide insulation. Such a baby is also at more risk for infection.
Very low birth weight babies (2 pounds or less) have an increased risk of developing cerebral palsy. Many causes of low birth weight are preventable with proper prenatal care.
Preterm

A newborn might also have a low birth weight if it is born at less than 37 weeks gestation, which qualifies it as a preterm baby (CDC, 2015, as cited in Paris et al., 2021). Early birth can be triggered by anything that disrupts the mother’s system. For instance, vaginal infections can lead to premature birth because such infection causes the mother to release anti-inflammatory chemicals which, in turn, can trigger contractions. Smoking and the use of other teratogens can lead to preterm birth. A significant consequence of preterm birth includes respiratory distress syndrome, which is characterized by weak and irregular breathing (see image).
Premature babies often cannot yet regulate their own temperature or feed by nursing or bottle. They may struggle to regulate their heart rate effectively and may experience jaundice. They often require care in the Neonatal Intensive Care Unit (NICU) until they are as healthy as a full-term baby.
Small-for-Date Infants

Infants that have birth weights that are below expectation based on their gestational age are referred to as small-for-date. These infants may be full term or preterm (see image below), but still weigh less than 90% of all babies of the same gestational age. This is a very serious situation for newborns as their growth was adversely affected. Regev et al. (2003, as cited in Paris et al., 2021) found that small-for-date infants died at rates more than four times higher than other infants.
Postmature
When babies are not born by 42 weeks gestation, or two weeks after their due date, they are considered overdue or postmature. There are some concerns about how long the placenta can function and most doctors will consider induction for overdue babies.
Stillborn
When a fetus (unborn baby) dies while still inside the mother (after 20-24 weeks gestation) or dies during delivery (childbirth), it is said that the delivered baby is stillborn. The causes of many stillbirths are unknown, even when special tests are done to learn the cause. Possible causes include: nicotine, alcohol, or drugs taken by the mother during pregnancy, physical trauma, radiation poisoning, Rh disease, and umbilical cord problems.
In 2019, there were 3,191 stillbirths in Canada. This is a fetal death rate of 8.6 per 1,000 total births (Statistics Canada, 2020).
Summary
- The mechanisms of heredity and genetic disorders.
- Elements of nature and nurture.
- The influence of nutrition and stress on development.
- Teratogens and their impact on prenatal development.
Next week we look at physical development of infants and toddlers.
References
Canadian Medical Association Journal. (2005, October 11). Diagnosis and treatment of etopic pregnancy. Retrieved from https://www.cmaj.ca/content/173/8/905
CYCCB. (n.d.). III. Applied Human Development. Retrieve from https://www.cyccb.org/competencies/applied-human-development
Diabetes Canada. (2022). Gestational diabetes. Retrieved from https://www.diabetes.ca/about-diabetes/gestational
Exner-Pirot, H., Norbye, B. & Butler, L. (Eds). (2018). Northern and indigenous health and health care. Retrieved from http://openpress.usask.ca/northernhealthcare
First Nations Centre, National Aboriginal Health Organization. (2009, December). Gestational diabetes and first nations women A literature review. Retrieved from https://fnim.sehc.com/getmedia/a7198c67-da87-44e9-9cc4-1d681303fef8/Gestational_Diabetes_LitReview_2009.pdf.aspx?ext=.pdf
Gurevich, R. (2020, April 20). Does age affect male fertility? Retrieved from https://www.verywellfamily.com/does-age-affect-male-fertility-1959934
Kenhteke Midwives. (2017). Welcome to Kenhteke midwives. Retrieved from https://kenhtekemidwives.com/#tab-id-4
Kolahdooz, F. , Launier, K., Nader, F. , Yi,K., Baker, P., McHugh, T., Vallianatos, H. and Sharma, S. (2016, September 2). Canadian indigenous womens perspectives of maternal health and health care services: A systematic review. Retrieved from https://diversityhealthcare.imedpub.com/canadian-indigenous-womens-perspectives-ofmaternal-health-and-health-care-services-asystematic-review.php?aid=11328
Lally, M. & Valentine-French, S. (2019). Lifespan development: A psychological perspective (2nd Ed). Retrieved from http://dept.clcillinois.edu/psy/LifespanDevelopment.pdf
Government of Canada. (2021). Canada Prenatal Nutrition Program: 25 years of success. Retrieved from https://www.canada.ca/en/public-health/services/publications/healthy-living/canada-prenatal-nutrition-program-25-years.html
Government of Ontario, (2021). Infant hearing program. Retrieved from https://www.ontario.ca/page/infant-hearing-program
Lumen Learning. (n.d.). Introduction to heredity, prenatal development and birth. Retrieved from https://courses.lumenlearning.com/lifespandevelopment2/chapter/lesson-3-heredity-prenatal-development-and-birth/
Mayo Clinic. (2022). Depression during pregnancy; You’re not alone. Retrieved from https://www.mayoclinic.org/healthy-lifestyle/pregnancy-week-by-week/in-depth/depression-during-pregnancy/art-20237875
OACYC. (2017). Code of Ethics. Retrieved from https://oacyc.org/code-of-ethics/
Pye, T., Scoffin, S., Quade, J., & Krieg, J. (2022). Child Growth and Development Canadian Ed. https://ecampusontario.pressbooks.pub/childgrowthanddevelopment/
Statistics Canada. (2020). Live births by marital status of the mother. Retrieved from https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310041901
Statistics Canada. (2018). Low birth weight babies by province and territory. Retrieved from https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310040401
Tantibanchachai, C. (2014, January 22). Teratogens. In the embryo project encyclopedia. Retrieved from https://embryo.asu.edu/pages/teratogens
Turkheimer, E. (2023). The nature-nurture question. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/tvz92edh
Weaver, I. (2023). Epigenetics in psychology. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/37p5cb8v
OER Attributions
Child Growth and Development Canadian Ed by Tanya Pye; Susan Scoffin; Janice Quade; and Jane Krieg is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Epigenetics in Psychology by Ian Weaver is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Lifespan Development by Lumen Learning is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
The Nature-Nurture Question by Eric Turkheimer is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
