Granulation
Incidence and Timing
We used the search terms “hypergranulation”, “hyper granulation”, “over growth”, and “over granulation” to find all postings related to granulation tissue around the stoma.
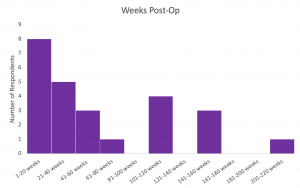
The duration of time since osseointegration surgery was reported by 25 persons; the median time of 38 weeks post-surgery (range: 6 weeks – 208 weeks). Most of the postings about granulation occurred in the first year post-OI with sporadic posts up to 4 years post-OI.
Symptoms
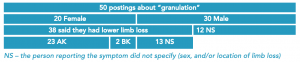
All responses were in regard to complaints of granulation or hypergranulation of tissue around the opening of their stoma. Two respondents indicated that their hypergranulation had occurred after changes made to their limb – one respondent had hypergranulation occur after having a dual cone replacement, and the other described hypergranulation after surgical alteration to their stoma. Another respondent indicated friction between the implant and stoma caused a build up of hypergranulation. Many of the respondents seemed to be dealing with chronic hypergranulation and had undergone several interventions for recurring granulation.
What People Have Tried
Several treatments or interventions were reported repeatedly in the postings related to granulation. Using silver nitrate to burn off the granulation was a common outcome for many of the respondents with several of them indicating that they had received silver nitrate treatments to burn off granulation on more than one occasion. One respondent reported using vaseline to protect healthy skin when burning off the granulation with silver nitrate. In some instances, granulated tissue was also removed with liquid nitrogen or surgery. Another common treatment reported for granulation was the use of steroid-type creams, such as Pimafucort (containing hydrocortisone), Kenacomb, Clobetasol propionate, and cortisone gel[1]. Other creams were listed as well including moisturizer-type creams such as Aveeno and antifungal creams like Resolve. In some cases, where granulation was recurrent, some respondents used numbing creams that contained lidocaine. Further, some respondents advised that to cut down on granulation, they used extra wound cleaning washes, such as Phisohex, Prontosan, Solosite gel, and/or saltwater washes. In general, many of the respondents also discussed using some type of lubrication around the stoma, mainly KY jelly and eye drops, though Vaseline and coconut oil were also mentioned.

Another common theme that was discussed at length was recurrent granulation and how to treat it. In many instances, continued use of the above creams/ointments or multiple treatments of silver nitrate were common. Some respondents also reported the granulated tissue tearing off on its own and some respondents reported actively trying to rip it off themselves. Mainly, the latter seemed to cause undue amounts of pain and was widely discouraged by other group members because of the pain it caused. One respondent reported they used a pressure wrap around the stoma to avoid hypergranulation. It was also noted that several respondents simply ignored the hypergranulation.
Fact Checker
[1] Topical steroids may decrease the rate of healing and increase the risk of infection. They should be used on open wounds only with the guidance of a health care professional (Marks, 1983). Most of the research on topical steroids and wound healing is older literature.
Help keep this resource alive.
Visit this Qualtrics link to fill out a survey on granulation so we can continue to grow the information and keep it up to date.