27 7.1 – Introduction and Background
Background of Crohn’s Disease

Inflammatory Bowel Disease (IBD) is a chronic inflammatory condition that includes Crohn’s disease (CD) and Ulcerative Colitis. This chapter focuses on relapsing CD and how it can lead to the formation of abdominal masses such as phlegmon and absecess. CD can affect any part of the intestines where it can cause severe abdominal pain, diarrhea, fatigue, weight loss and malnutrition. So far, the exact etiology of CD is still unknown, some studies showed that diet and stress were the leading cause of the disease. More recent studies illustrates that there are number of other factors such as, genetic, , environmental factors, luminal microbial antigens, ethnic origin and deregulated immune system (Baumgart, 2007), can have huge influences on the gastrointestinal tracts with its ability to distinguish foreign from self-antigens. In terms of the infection sites, the terminal and the right colon are the most commonly involved site but this pathological and clinical disorder can affect any part of the GI tracts and in all layers of intestinal wall.
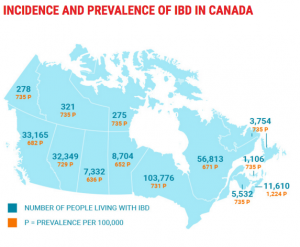
Statistically, approximately 270,000 Canadians are living with with IBD and it is expecting to rise to 400,000 by the end of 2030. Studies shown that IBD is more common in adults than in children. People are most often diagnosed with CD and UC in early adulthood however, the diagnosis can still happen at any age period. Generally, CD is more prominent in women than men, while ulcerative colitis is more common in men than women.
Introduction
The current treatment is very much limited and there are many clinical challenges in order to maintain the recurrence of CD. Small inflammatory masses can definitely be treated with high dose of steroid or anti-TNF therapy along with proper antibiotics coverages however, it may not prevent for the need for treatment. (Feagins et. al, 2011 & Lichtenstein et. al, 2009). Surgical resection can be done to treat small inflammatory masses but they are inevitable for refractory cases. Consequently, due to the postoperative recurrence of the CD and short bowel syndrome resulting from multiple surgeries, surgical operations are considered as a last line of treatment.
The fact that the management of refractory CD complicated with intra abdominal inflammatory mass is very challenging, the author propose a multiple Fecal Microbiota Transplant (FMT) as an alternate source of treatment. A concept originated in ancient chinese literature supported by recent their preliminary studies, shows a promising method of treatment for inflammatory bowel disease. Ultimately, this paper aims to evaluate the efficacy and safety of multiple FMT for treating CD with intra abdominal inflammatory mass. The authors hypothesized that multiple fresh FMT could potentially induce clinical remission and moreover, multiple repeated treatment of FMT could maintain the remission of Crohn’s disease.