10.3 Nasogastric Tubes
Using a Nasogastric Tube
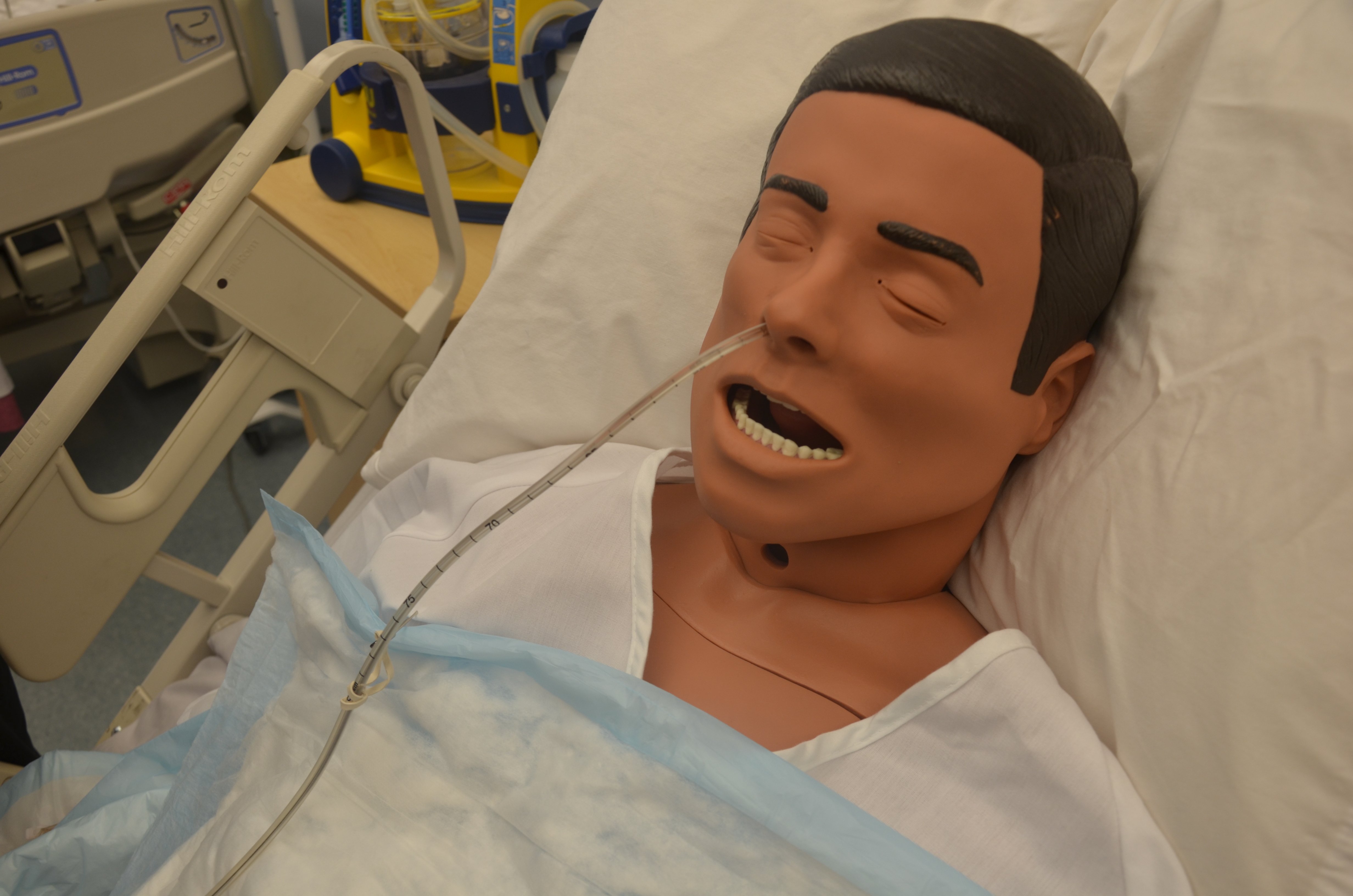
A nasogastric (NG) tube is a flexible plastic tube inserted through the nostrils, down the nasopharynx, and into the stomach or the upper portion of the small intestine. Placement of NG tubes is always confirmed with an X-ray prior to use (Perry, Potter, & Ostendorf, 2014).
NG tubes are used to:
- Deliver nutrients to the patient via a feeding pump
- Remove gastric contents
An NG tube used for feeding should be labelled. The tube is used to feed patients who may have swallowing difficulties or require additional nutritional supplements. These tubes are narrower and smaller bored than a Salem sump or Levine tube.
An NG tube can also remove gastric content, either draining the stomach by gravity or by being connected to a suction pump. In these situations, the NG tube is used to prevent nausea, vomiting, or gastric distension, or to wash the stomach of toxins.
The NG tube is fastened to the patient using a nose clip, and is taped and pinned to the patient’s gown to prevent accidental removal of the tube and to prevent the tube from slipping from the stomach area into the lungs.
When working with people who have nasogastric tubes, remember the following care measures:
- Maintain and promote comfort. The tube constantly irritates the nasal mucosa, causing a great deal of discomfort. Ensure that the tube is securely anchored to the patient’s nose to prevent excess tube movement, and is pinned to the gown to avoid excessive pulling or dragging.
- Because one nostril is blocked, patients tend to mouth breathe. This causes dehydration of the nasal and oral mucosa, and patients will complain of thirst, but they are usually NPO (nil per os or nothing by mouth). Mouth care will help to relieve the dryness. This can include rinsing the mouth with cold water or mouthwash as long as the patient does not swallow. Some patients may be allowed to suck on ice chips.
- If the patient complains of abdominal pain, discomfort, or nausea, or begins to vomit, report it immediately. The drainage flow is probably obstructed and the tube will need to be irrigated.
- These patients should never be allowed to lie completely flat. Lying flat increases the patient’s risk of aspirating stomach contents. Patients with an NG tube are at risk for aspiration. The head of bed should always be raised 30 degrees or higher.
Checklist 78 outlines the steps for inserting a nasogastric tube.
Checklist 78: Inserting a Nasogastric tubeDisclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
| Steps | Additional Information | ||
|---|---|---|---|
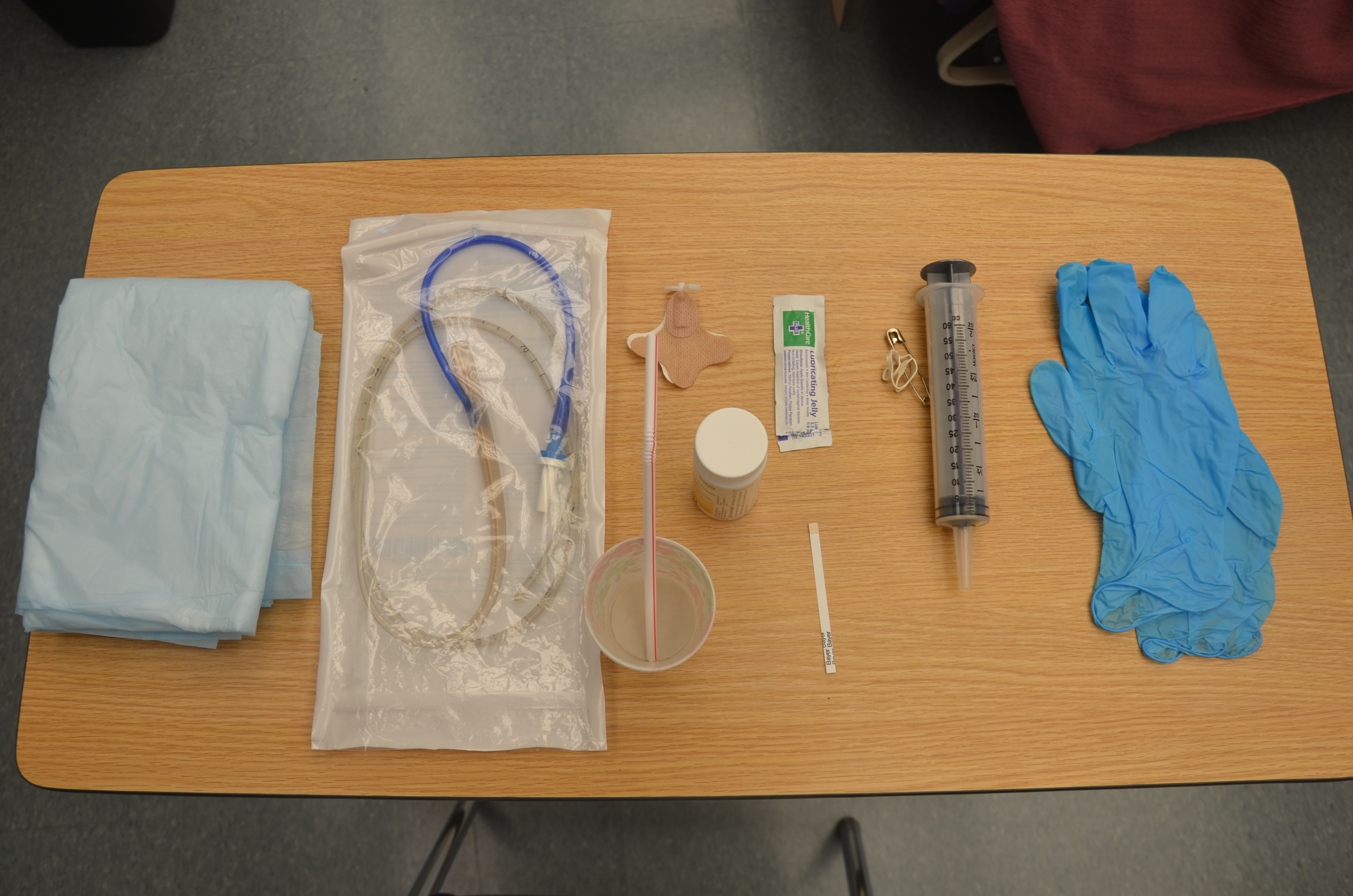
| 1. Perform hand hygiene and gather supplies. | This prevents the transmission of microorganisms.
 |
||
| 2. Visually inspect condition of patient’s nasal and oral cavities. | Check for signs of infection or skin breakdown. | ||
| 3. Assess for the best nostril before you begin.
Do this by occluding one side and asking the patient to sniff. Ask the patient about previous injuries or history of a deviated septum. |
If either nostril is equally suitable, select the nostril closest to the suction.
 |
||
| 4. Palpate patient’s abdomen for distension, pain, and/or rigidity.
Auscultate for bowel sounds. |
Document assessment findings and determine appropriateness of NG tube insertion related to reason for insertion and patient’s physical assessment. | ||
| 5. Assess patient’s level of consciousness and understanding of procedure. | Patient must be able to follow instructions related to NG insertion to allow for passage of tube through nasal and gastrointestinal tracts. | ||
| 6. Check doctor’s orders for type of NG tube to be placed and reason for placement. | Check appropriate orders relevant to patient safety. | ||
| 7. Check doctor’s orders to determine whether the NG tube is to be attached to suction or a drainage bag. | This should be commensurate with the reason for the NG tube. | ||
| 8. Position patient sitting up at 45 to 90 degrees (unless contraindicated by the patient’s condition), with a pillow under the head and shoulders. | This allows the NG tube to pass more easily through the nasopharynx and into the stomach. | ||
| 9. Raise bed to a comfortable working height. | This helps prevent biomechanical injury to the health care provider. | ||
| 10. Agree on a signal the patient can use if they wish you to pause during the procedure. | This procedure can be anxiety-provoking and uncomfortable for many patients. Providing a means for the patient to communicate discomfort and a desire to pause during the procedure helps alleviate anxiety. | ||
| 11. Place a towel on the patient’s chest and provide facial tissues and an emesis basin. | Nasal and oral secretions may be evident during the procedure. | ||
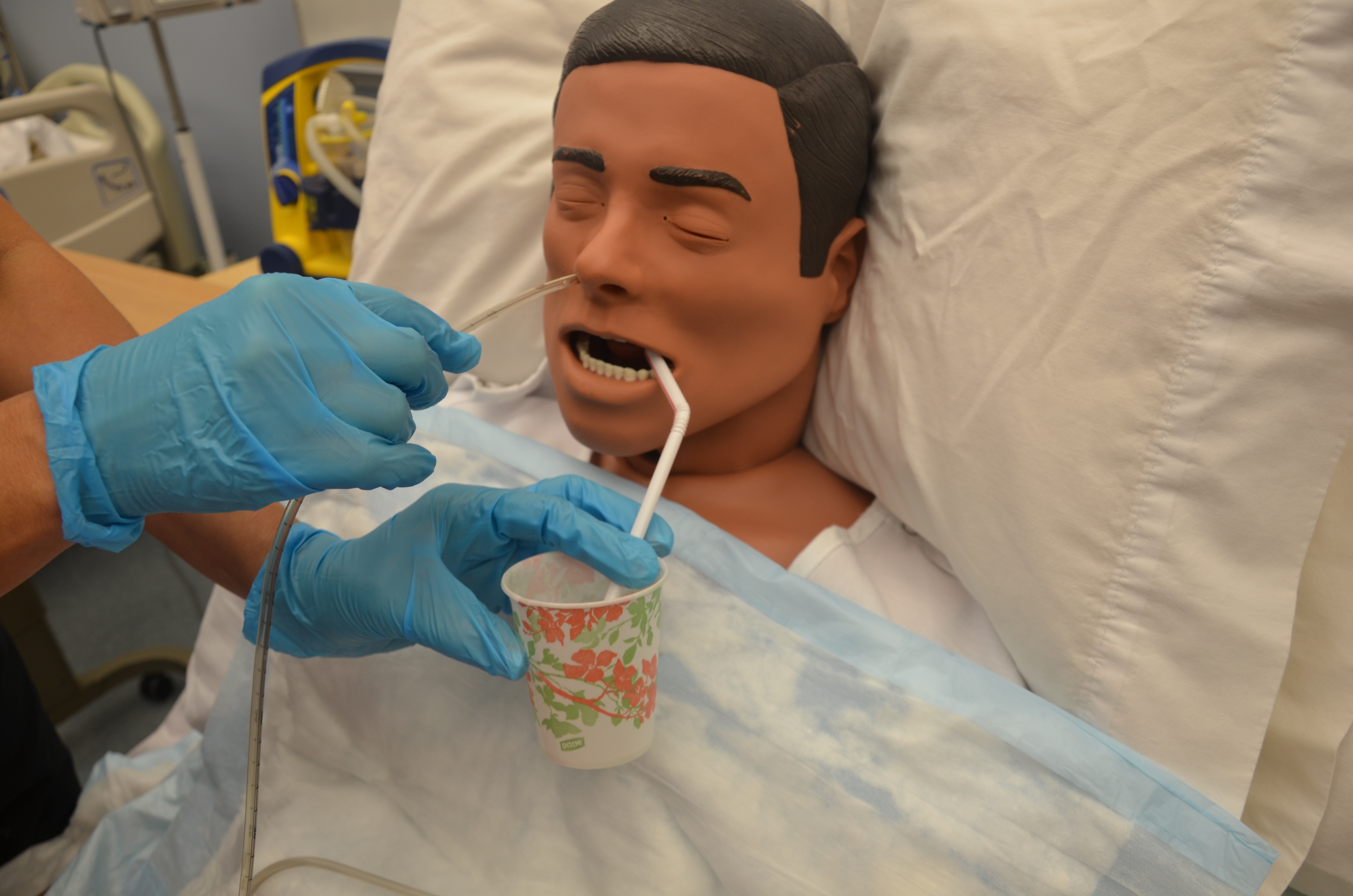
| 12. Provide patient with drinking water and a straw if the patient is not fluid restricted. | Sipping water through a straw helps to initiate the swallowing reflex and facilitate passing of NG tube. | ||
| 13. Stand on patient’s right side if you are right-handed and the left side if you are left-handed. | You will use your dominant hand to insert the tube. | ||
14. Measure distance of the tube from
and then mark the tube at this point.
|
This determines the appropriate length of NG tube to be inserted.
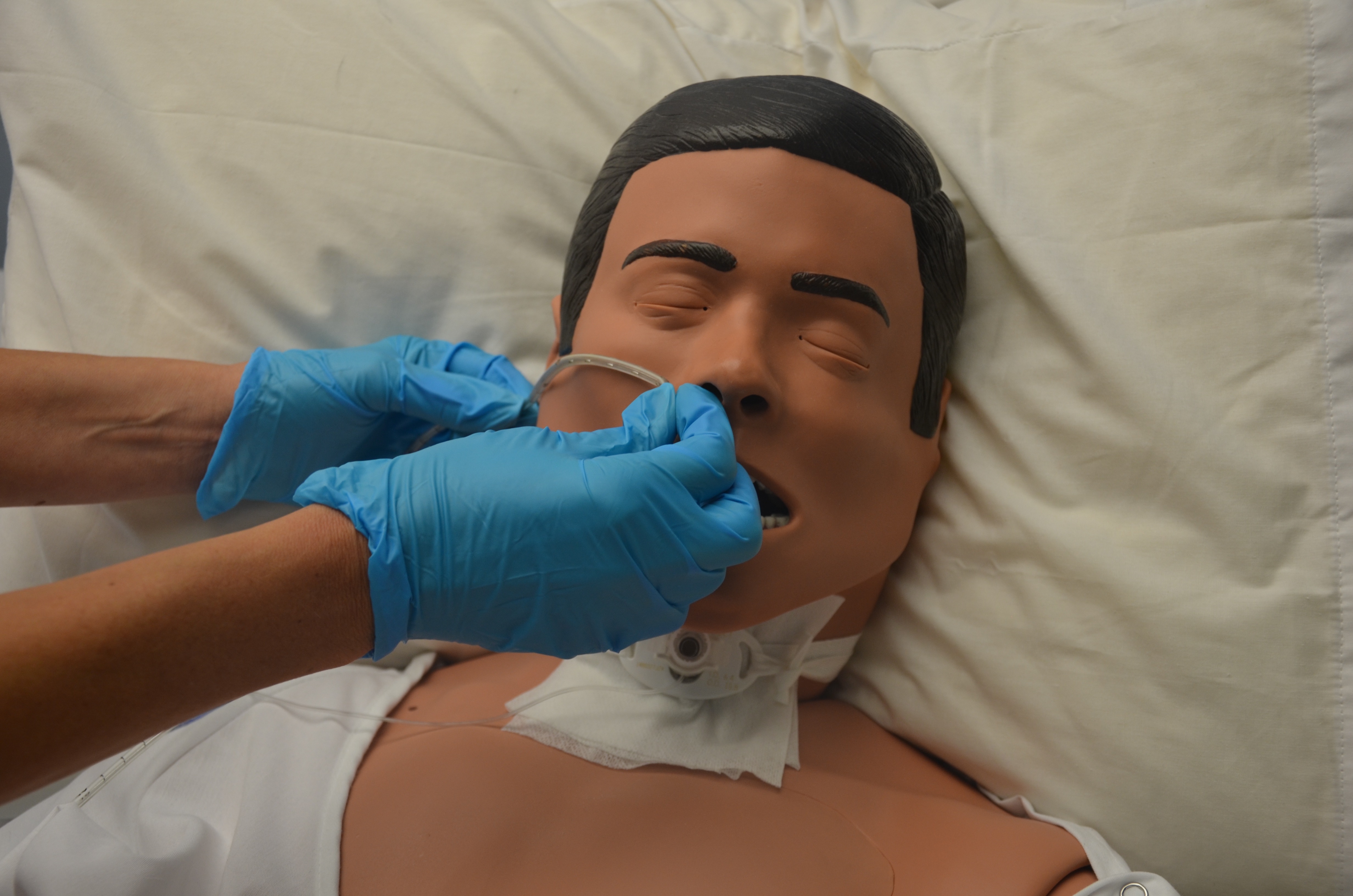  |
||
| 15. Lubricate NG tube tip according to your agency policy. | Tube may be lubricated internally using tap water or externally using water-soluble lubricating jelly. Agency policy varies and should be checked.
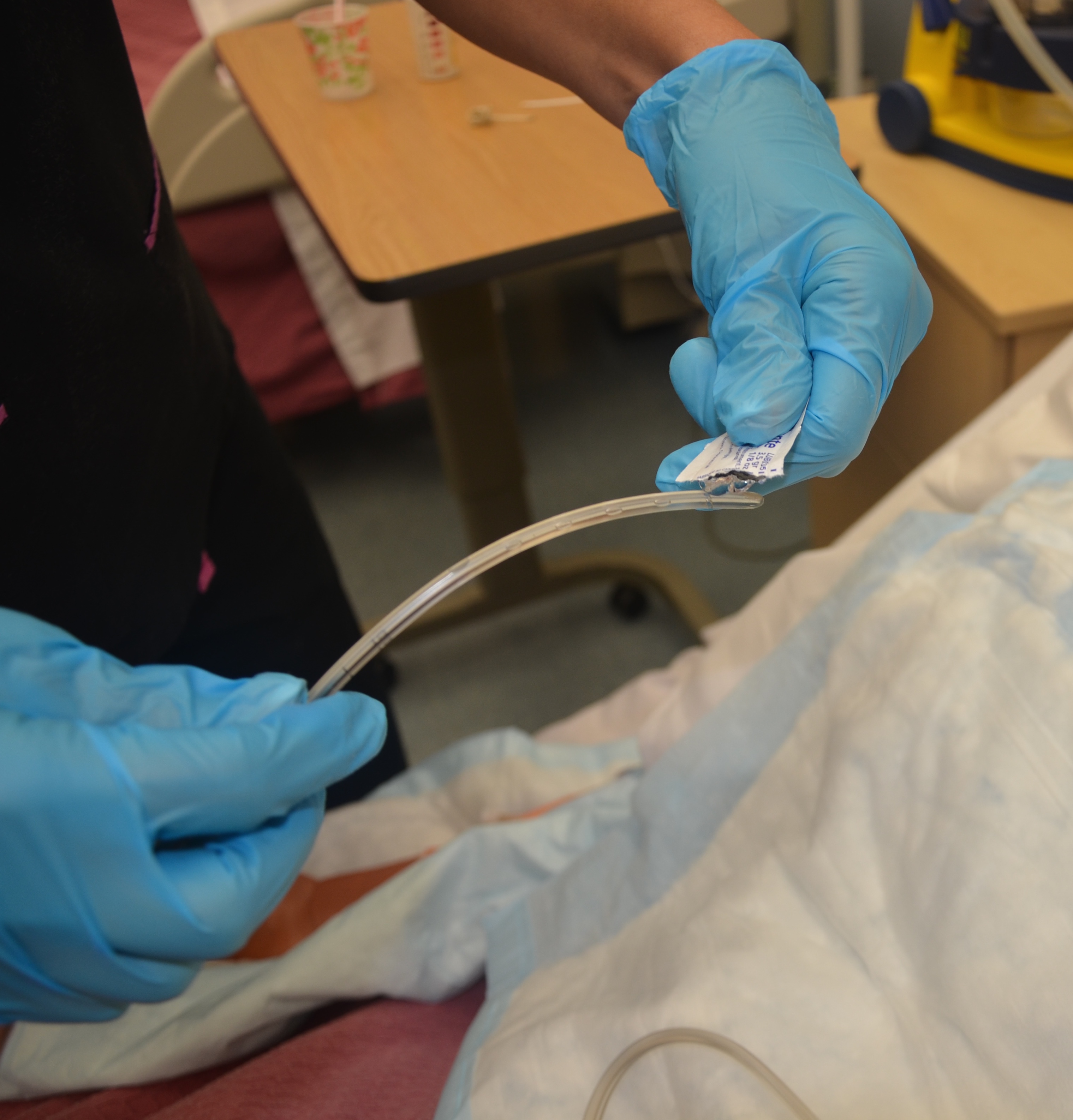 Never use non-water-soluble lubricant (e.g., Vaseline), as it will not dissolve and may cause respiratory complications if it enters the lungs. |
||
| 16. Apply clean non-sterile gloves. | Using gloves decreases the transfer of microorganisms.
 |
||
| 17. Curve 10 to 15 cm of the end of the NG tube around your gloved finger, and then release it. | Curling the NG tube around your finger helps it conform to the normal curve of the nasopharynx.
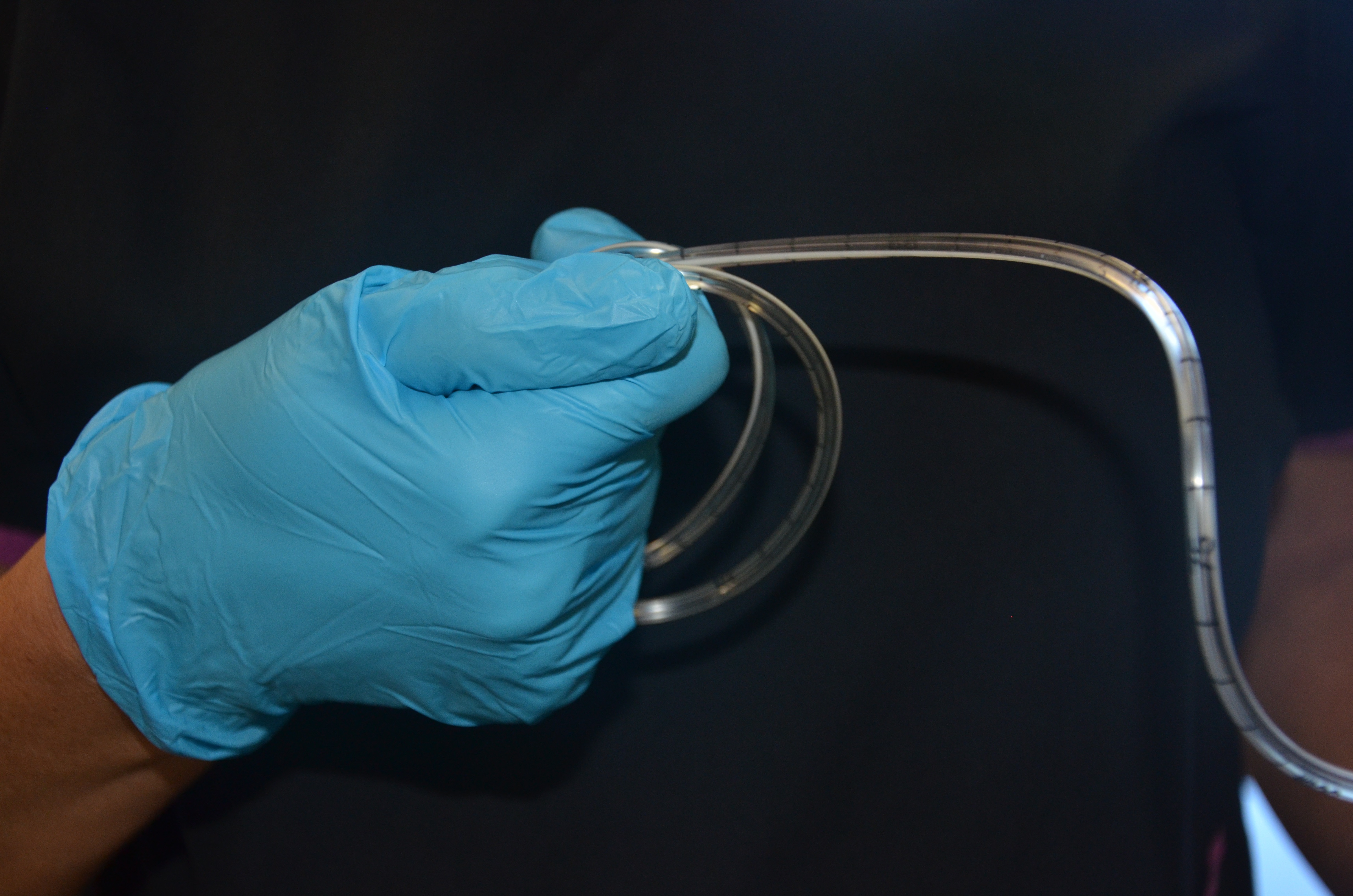 |
||
| 18. Have patient drop head forward and breathe through the mouth. | Dropping the head forward closes the trachea and opens the esophagus, which allows the NG tube to pass more easily through the nasopharynx and into the stomach. | ||
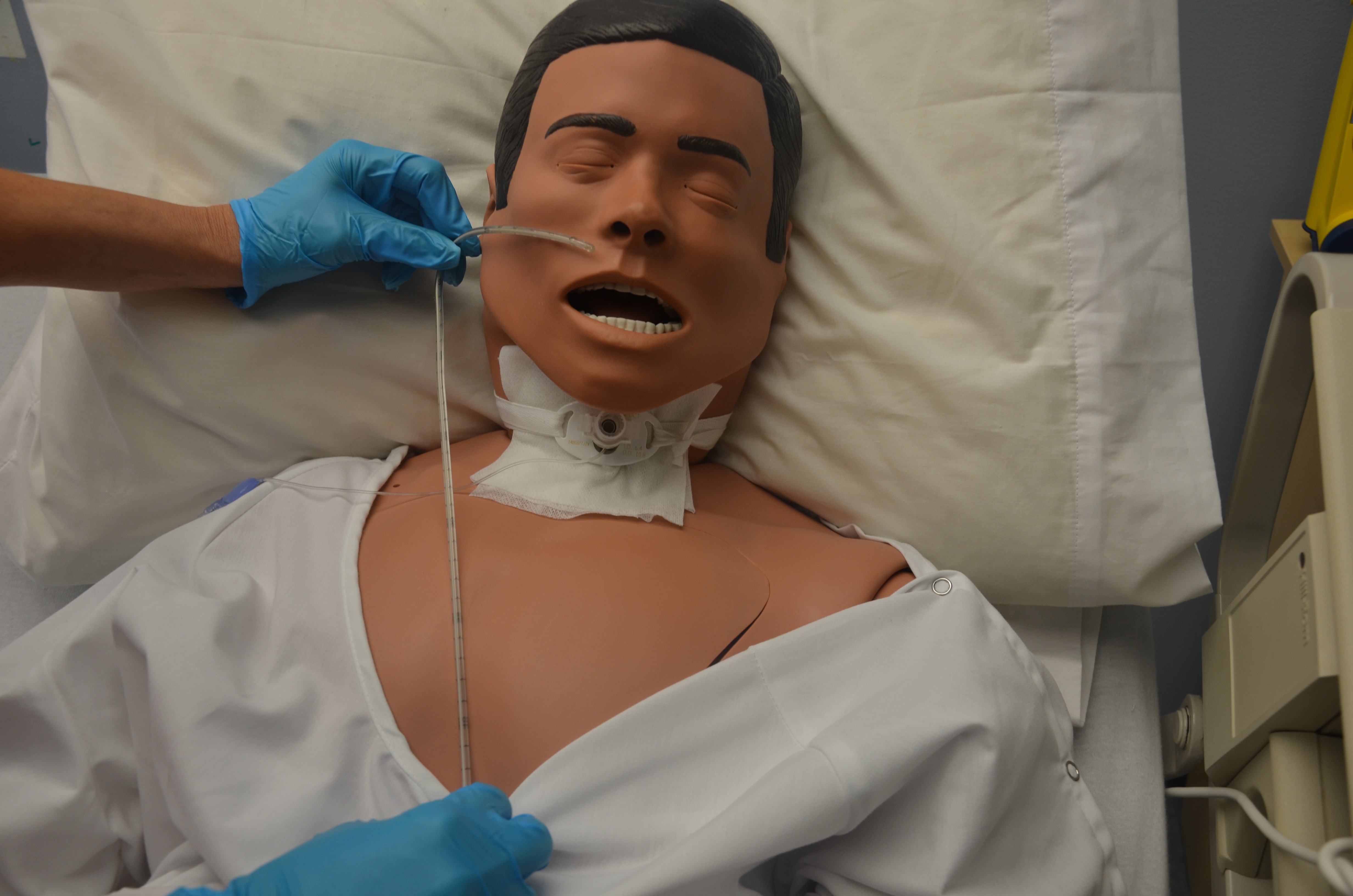
| 19. Insert NG tube tip slowly into the patient’s nostril and advance it steadily, in a downward direction, along the bottom of the nasal passage, with the curved end pointing downward in the direction of the ear on the same side as the nostril. | This follows the natural anatomical alignment of the nasopharynx.
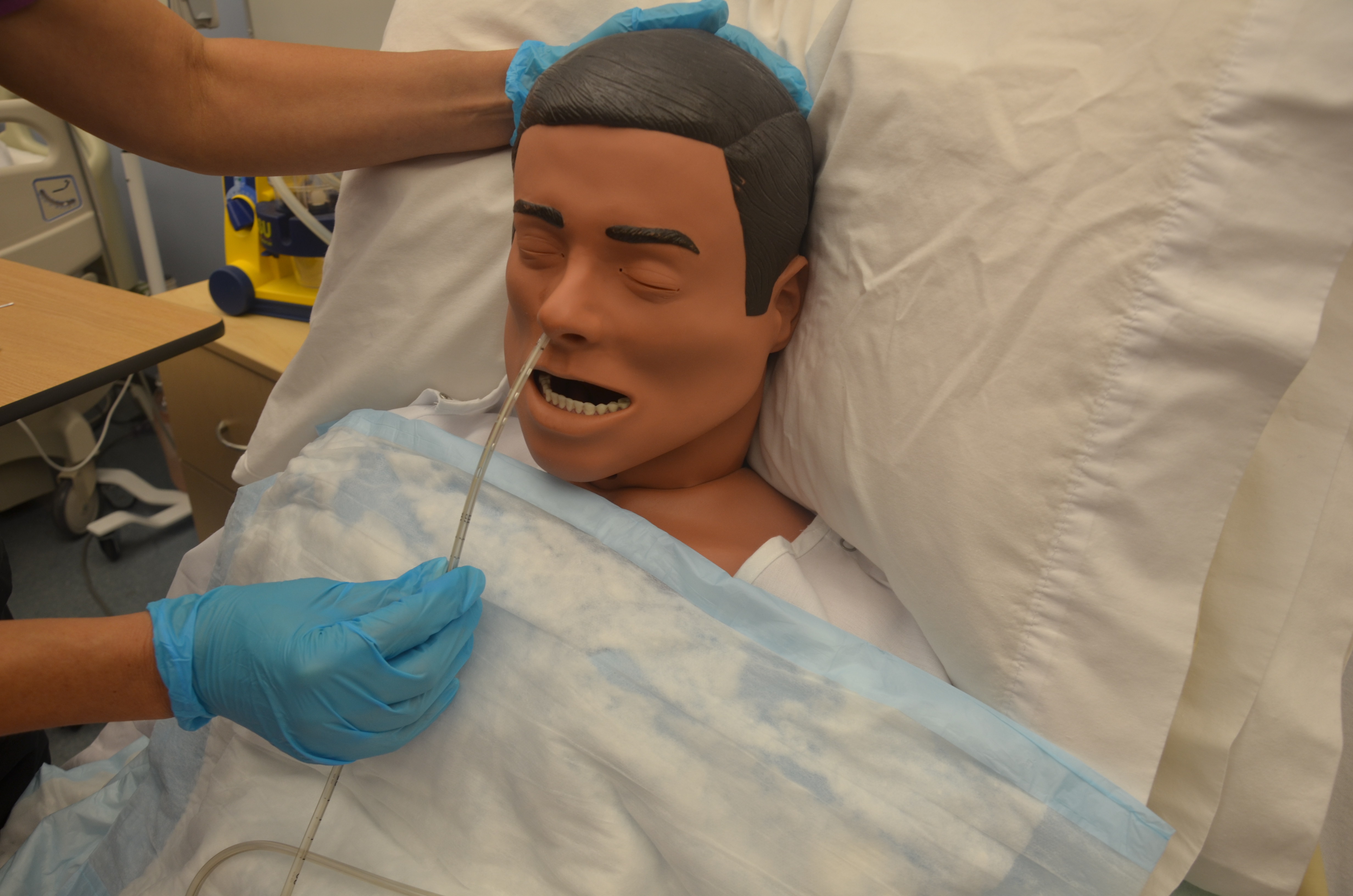 |
||
| 20. You may feel slight resistance as you advance along the nasal passage. Twist the tube slightly, apply downward pressure, and continue trying to advance the tube. If significant resistance is felt, remove the tube and allow the patient to rest before trying again in the other nostril. | It is common for the patient to feel discomfort, and this may be expressed with light coughing and gagging. More aggressive coughing and gagging may indicate that the tube has entered the airways, in which case you should withdraw the NG tube.
 |
||
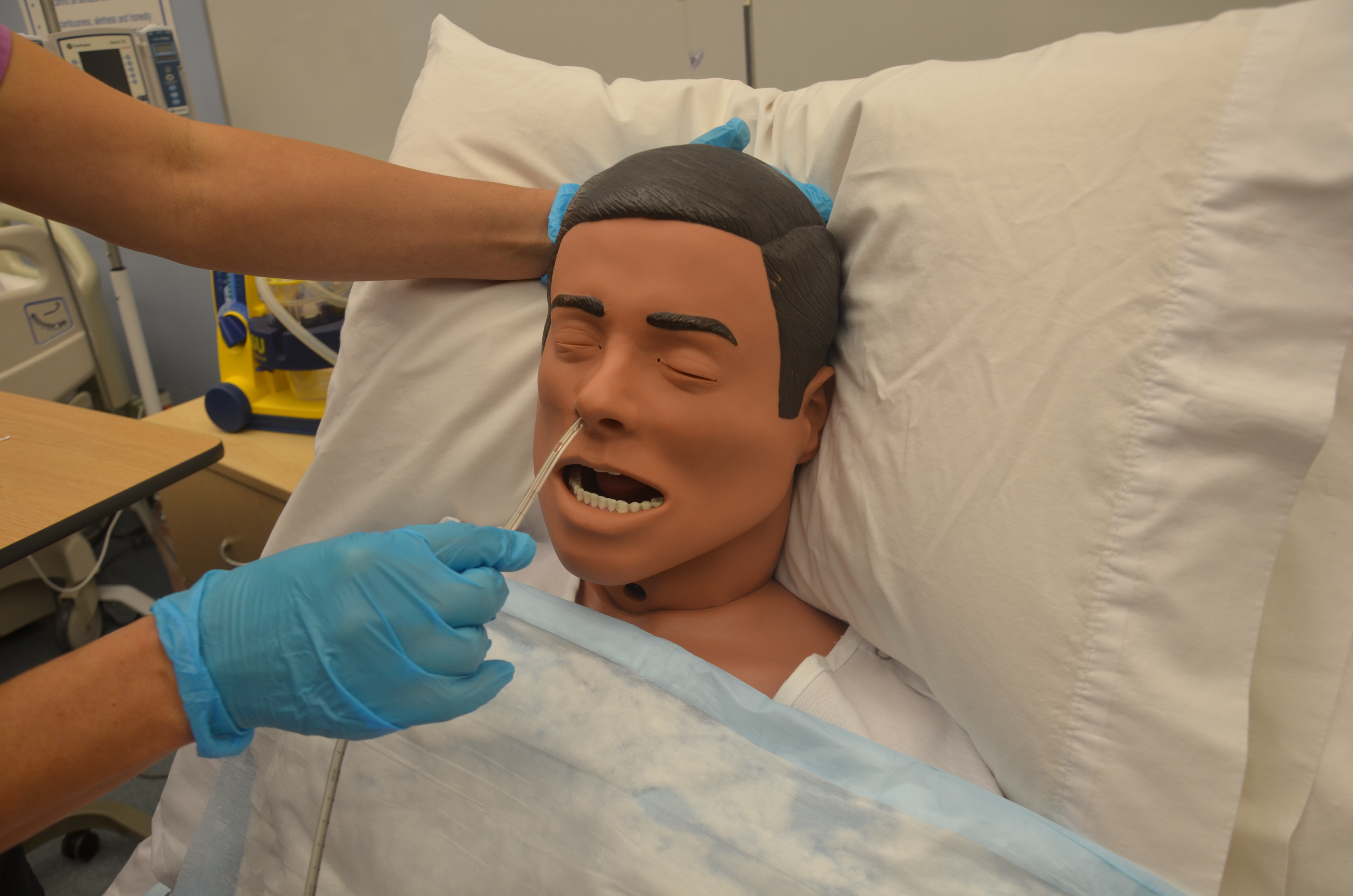
| 21. If there is difficulty in passing the NG tube, you may ask the patient to sip water slowly through a straw unless oral fluids are contraindicated. If oral fluids are not allowed, ask the patient to try dry swallowing while you advance the tube. | If patient continues to gag or cough, check that the tube is not coiled in the back of the mouth, using a tongue blade and a flashlight to check the back of the mouth. If tube is coiled, withdraw the tube until only the tip of the tube is seen in the back of the mouth. Then try advancing the tube again while patient tries to swallow.
 |
||
| 22. Continue to advance NG tube until you reach the mark/tape you had placed for measurement. | This ensures accurate placement. | ||
| 23. Temporarily anchor the tube to patient’s cheek with a piece of tape until you can check for correct placement. | This prevents displacement of the NG tube while checking placement.
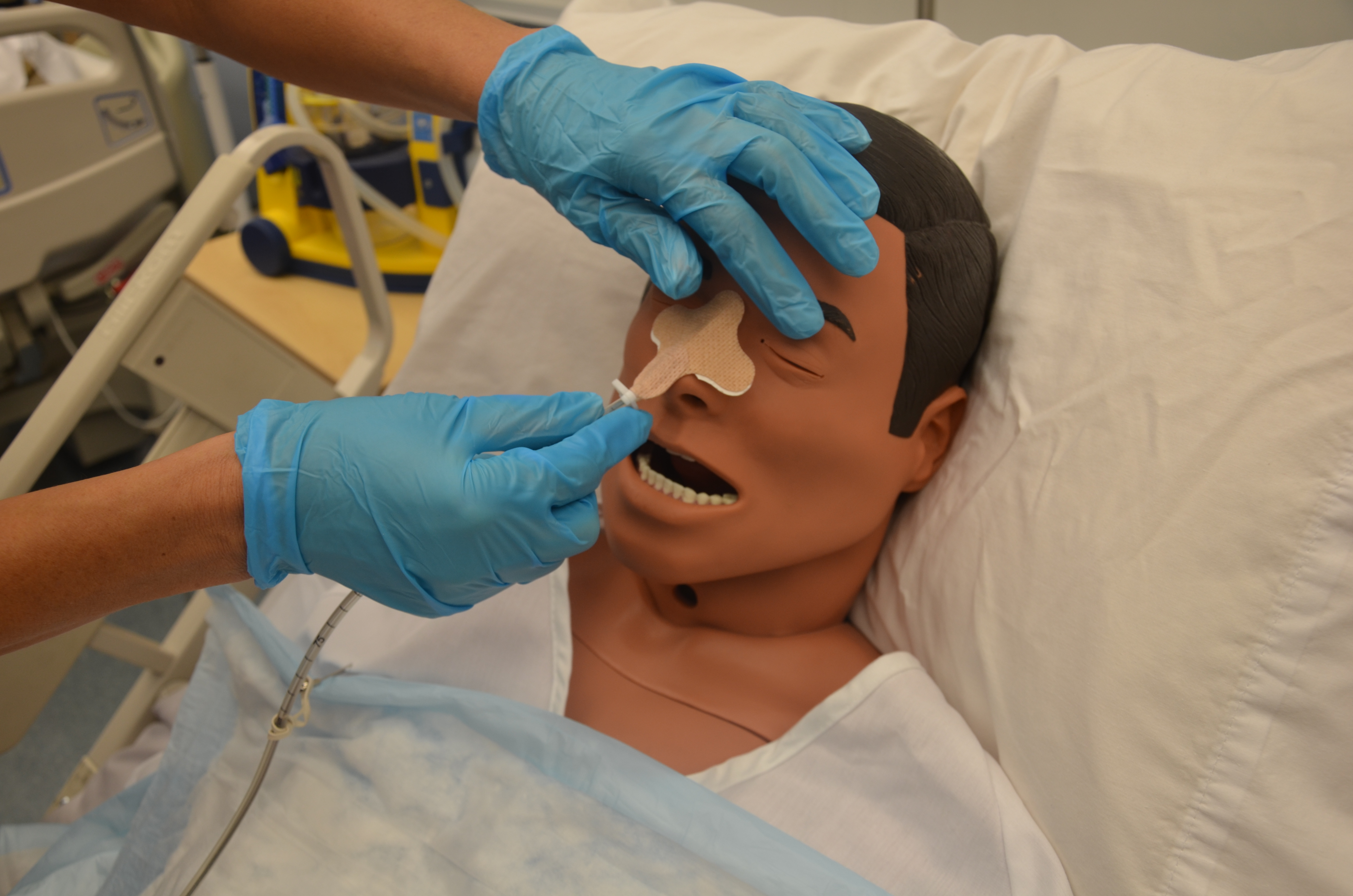 |
||
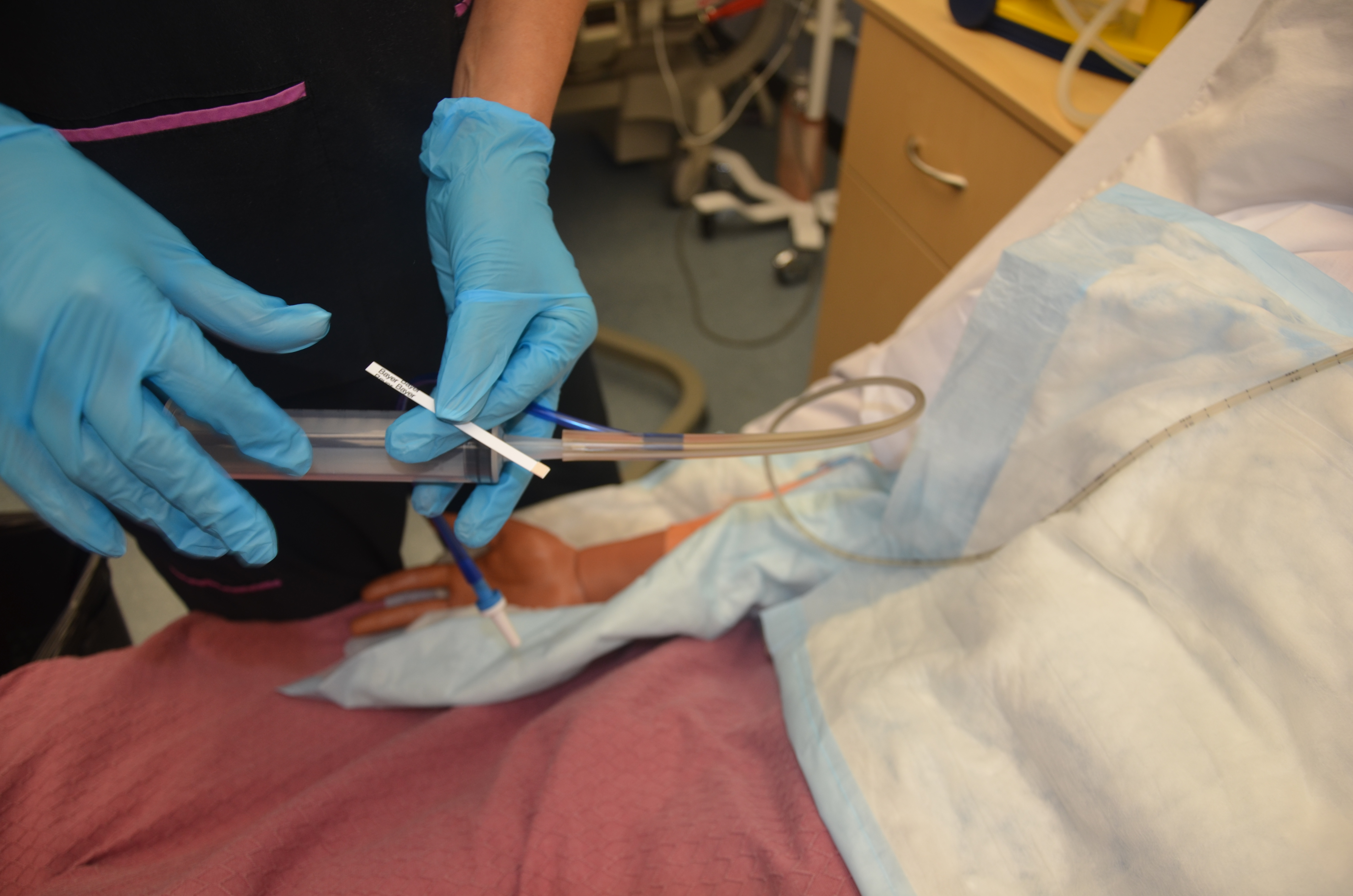
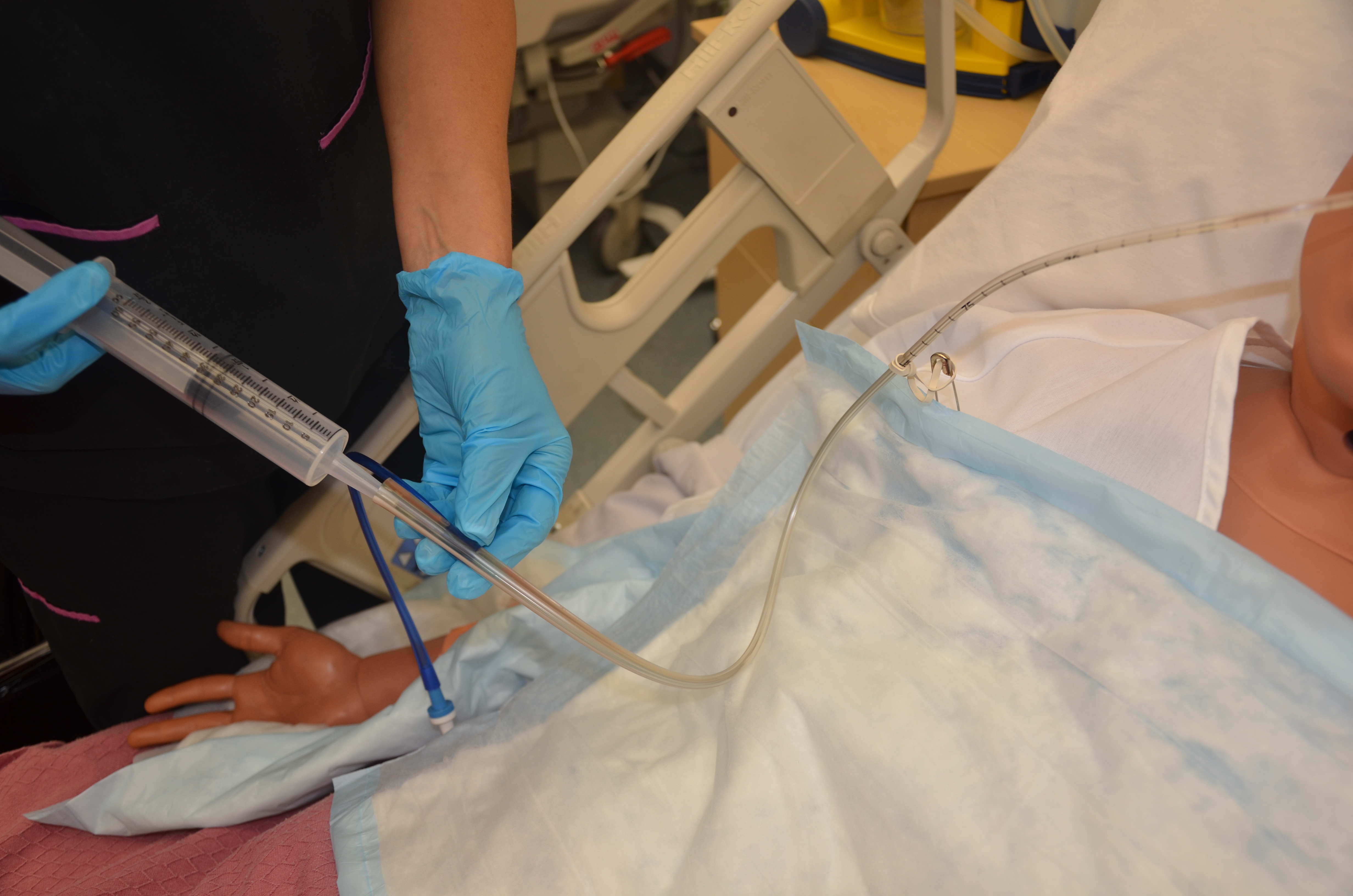
| 24. Verify tube placement according to agency policy.
Colour-coded pH paper is usually used, as an initial and interim check, to confirm that acidic contents are present. Then an X-ray is taken to confirm placement prior to using NG tube for feeding. |
The contents aspirated from the tube should be acidic with a pH <5. If the pH is more than 6, it may indicate the presence of respiratory fluids or small bowel content, and the tube should be removed.
 |
||
| 25. Once the tube placement has been confirmed, mark (with a permanent marker) and record the length of tubing extending from the nose to the outer end of the tube. | This aids in timely recognition and identification of tube displacement or migration. | ||
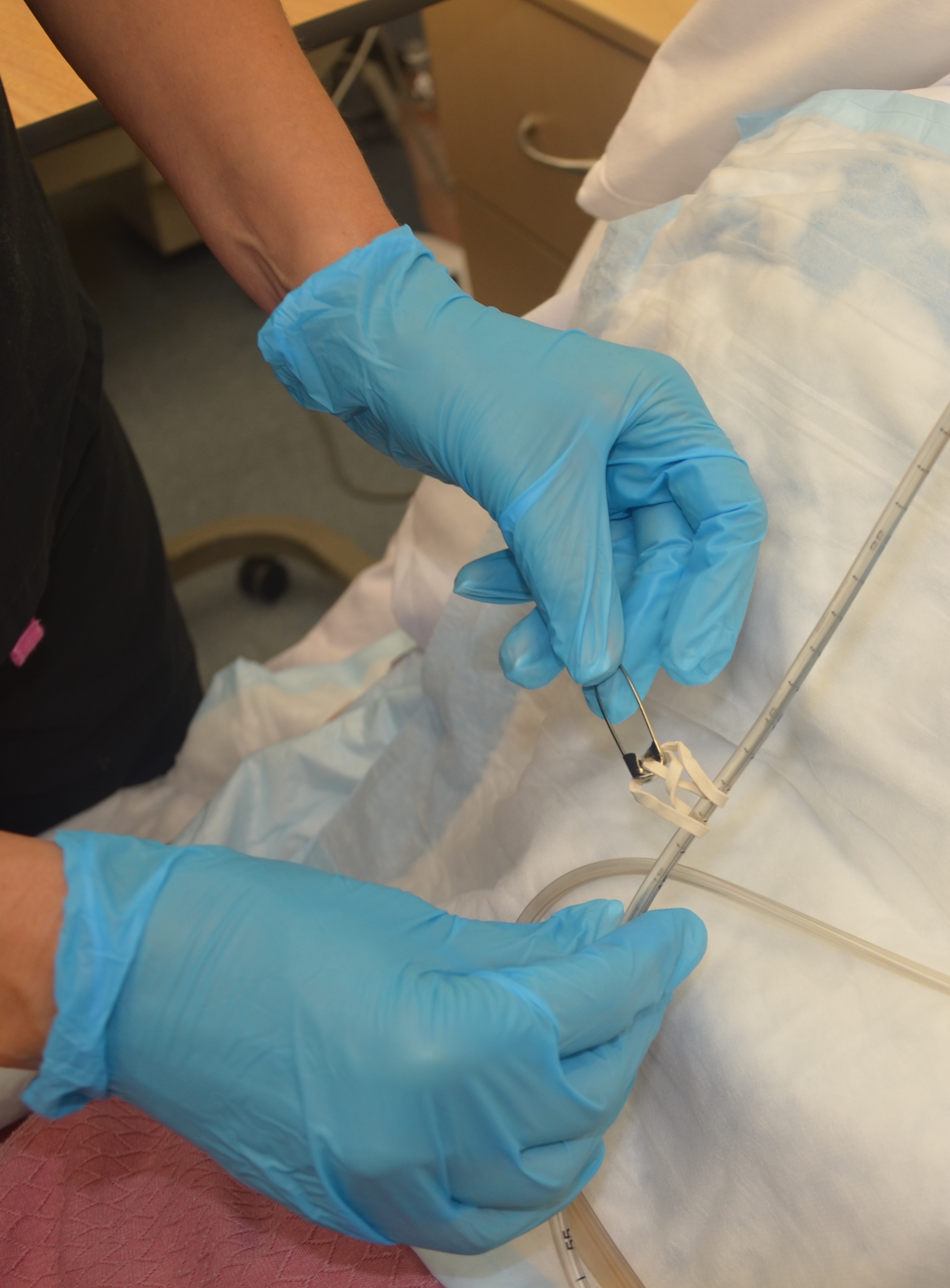
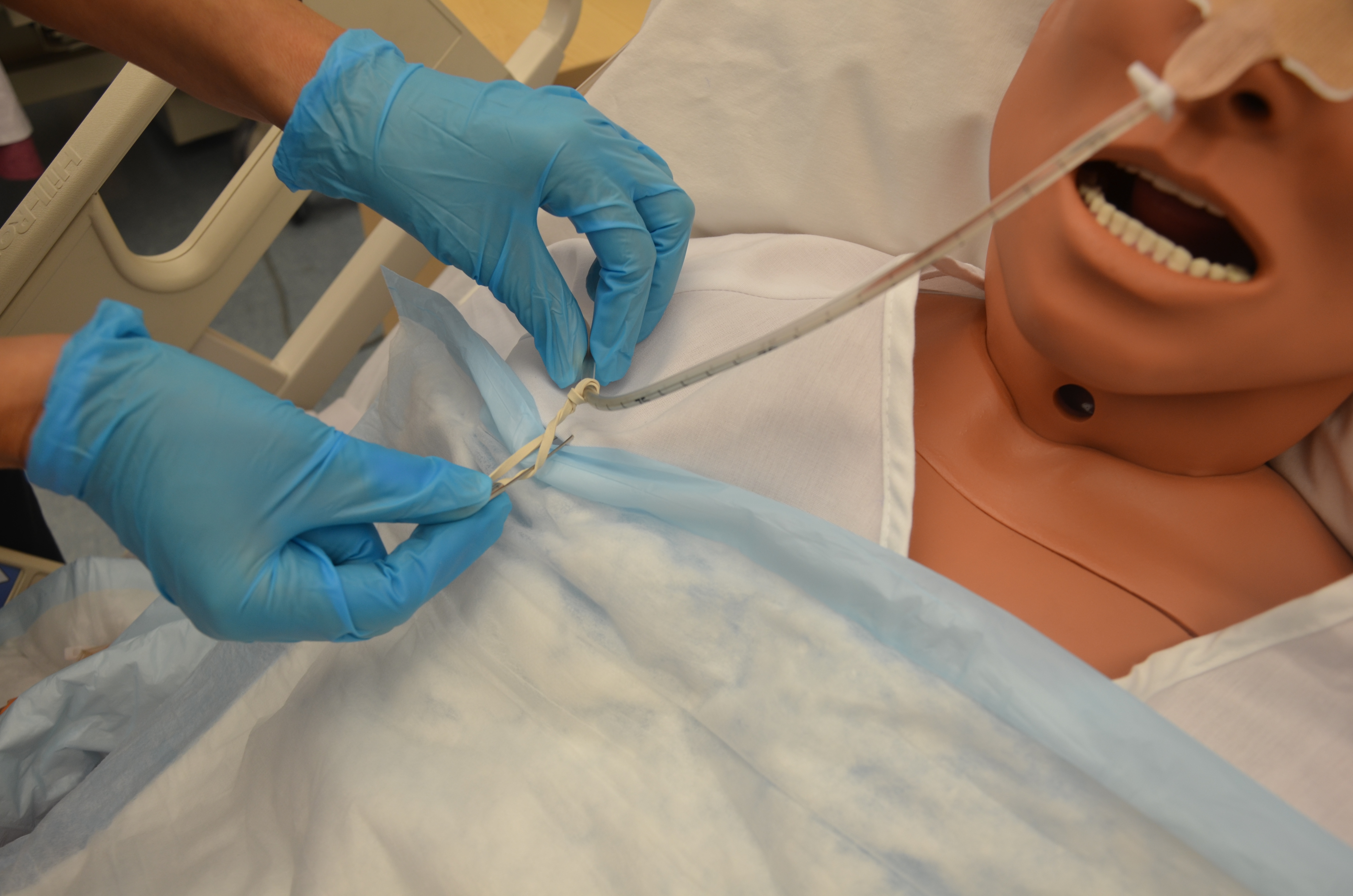
| 26. Secure the tube to the patient’s gown with a safety pin, allowing enough tube length for comfortable head movement. | This keeps the NG tube in place.
 |
||
| 27. Document the procedure according to agency policy, and report any unexpected findings to the appropriate health care provider. | Timely and accurate documentation promotes patient safety. | ||
| Data source: ATI, 2015a; BCIT, 2015c; Berman & Snyder, 2016 | |||
Special considerations with NG tubes:
- Always assess correct placement of the NG tube prior to infusing any fluids or tube feeds as per agency policy. Check location of external markings on the tube and colour of the PH of fluid aspirated from the tube. Routine evaluation will ensure the correct placement of the tube and reduce the risk of aspiration. Do not instill air to test location of tube.
- Do not give the patient anything to eat or drink without knowing that the patient has passed a swallowing assessment.
- If changing the gown or repositioning the patient, take care not to pull on the NG tube. Remember to unpin the tube from the gown and repin the tube.
- If the NG tube falls out of the patient, it is not an emergency. But be sure to assess your patient. How are the ABCCS? Notify the RN in charge of the patient.
- A patient who appears to be in respiratory distress should be considered an emergency, and emergency procedures should be followed. Respiratory distress may present as coughing, choking, or reduced oxygen saturation.
Removing an NG Tube
An NG tube should be removed if it is no longer required. The process of removal is usually very quick. Prior to removing an NG tube, verify physician orders. If the NG tube was ordered to remove gastric content, the physician’s order may state to “trial” clamping the tube for a number of hours to see if the patient tolerates its removal. During the trial, the patient should not experience any nausea, vomiting, or abdominal distension.
To review how to remove an NG tube, refer to Checklist 79.
Checklist 79: Removal of an NG TubeDisclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
| Steps | Additional Information | ||
|---|---|---|---|
| 1. Verify health care provider’s orders to remove NG tube. | An order is required to remove an NG tube. | ||
| 2. Collect supplies. | Supplies include waterproof pads, 20 ml syringe, tissues, non-sterile gloves, and garbage bag. | ||
| 3. Verify patient using two identifiers. Explain procedure to patient and place patient in high Fowler’s position. | Follow agency policy for proper patient identification. | ||
| 4. Perform hand hygiene. Place waterproof pad on patient’s chest. | This reduces the transmission of microorganisms.
 |
||
| 5. Disconnect tube from feed if present. | This prevents risk of aspiration of tube feed.
 |
||
| 6. Remove tape or securement device from nose. | This allows for the tube to be easily removed.
 |
||
| 7. Unclip NG tube from patient’s gown. | This allows for tube to be easily removed.
 |
||
| 8. Clear NG tube by inserting 10 to 20 ml of air into tube. | This prevents aspiration of tube feed falling out of tube.
 |
||
| 9. Instruct patient to take a deep breath and hold it. | This prevents aspiration; holding the breath closes the glottis. | ||
| 10. Kink the NG tube near the naris and gently pull out tube in a swift, steady motion, wrapping it in your hand as it is being pulled out. Dispose of tube in garbage bag. | This prevents any residual feed from flowing out of tube upon removal.

 |
||
| 11. Offer tissue or clean the nares for the patient and offer mouth care as required. | This clears the nares/nasal passages of any remaining secretions.
|
||
| 12. Remove gloves and place patient in a comfortable position. Assess patient’s level of comfort. Perform hand hygiene. | This promotes patient comfort and reduces the transmission of microorganisms.
 |
||
| 13. Document procedure according to agency policy | Document removal of NG tube and patient response to the removal. | ||
| Data source: ATI, 2015a; BCIT, 2015b; Perry et al., 2014 | |||
Critical Thinking Exercises
- You are inserting a nasogastric tube and the tube is not advancing. Explain your next steps, with rationale.
- Your patient has a nasogastric tube and is requesting water because her throat feels dry. Describe your next actions.
