9.8 Current Harm Reduction Prevention Programs
Harm Reduction Learning Outcomes
In this chapter we examine a variety of Harm Reduction Prevention Programs
- What is harm reduction
- Discuss the purpose of harm reduction
- Explain the challenges in harm reduction
- Discuss 3 different harm reduction strategies or programs
What is harm reduction
Harm reduction, based on the definition by the International Harm Reduction Association (2021) is stated as “policies, programmes and projects that aim to reduce the health, social and economic harms associated with the use of psychoactive substances. It is an evidence-based and cost-effective approach – bringing benefits to the individual, community and society” (1). In Canada, harm reduction programs are heavily dependent on community-based agencies and reliant on provincial and federal government funding for service provision, so lack consistency. In 2015, “only two jurisdictions in Canada had current provincial-level, stand-alone harm reduction policies” (2), which confirms what many individuals working in harm reduction in Canada have suggested, that a harm reduction philosophy is not embedded in policy or funding at any governmental level.

Harm Reduction is applied different for everyone
There are a variety of agencies that address substance use, from the Government of Canada, correctional facilities, Public Health, Canadian Centre on Substance Abuse, The Centre for Addiction and Mental Health, National Native Alcohol and Drug Abuse Program, and various health authorities, private agencies, and businesses as well as non-governmental organizations across the country. Each of these agencies have a mandate to address substance use in some way, from individual treatment through to incarceration. Each of these agencies focuses on substance use differently, some recognizing the intersectionality of substance use while others do not. Part of the work of Social workers is to address the stigma associated not only with substance abuse but also with harm reduction. How can this be done?
Why is harm reduction important? Effective harm reduction programs seek to serve some of the most marginalized individuals in our country. Please watch the video below to further understand harm reduction in Canada. We have explored, substance use is frequently misunderstood and stigmatized; therefore it stands to reason that harm reduction strategies that help support individuals who use substances would be concurrently maligned and perhaps not overtly supported in Canada. Part of your work, as Social workers, is to address the stigma associated with not only substance abuse, but harm reduction. How will you do thy is harm reduction important? Effective harm reduction programs seek to serve some of the most marginalized individuals in our country.
According to the Canadian Mental Health Association
Harm Reduction is an evidence-based, client-centred approach that seeks to reduce the health and social harms associated with addiction and substance use, without necessarily requiring people who use substances from abstaining or stopping.
#SupplyOrWeDie – Toronto Harm Reduction Alliance. By Toronto Harm Reduction Alliance. Join the movement for a safe supply of drugs (4)
Transcript
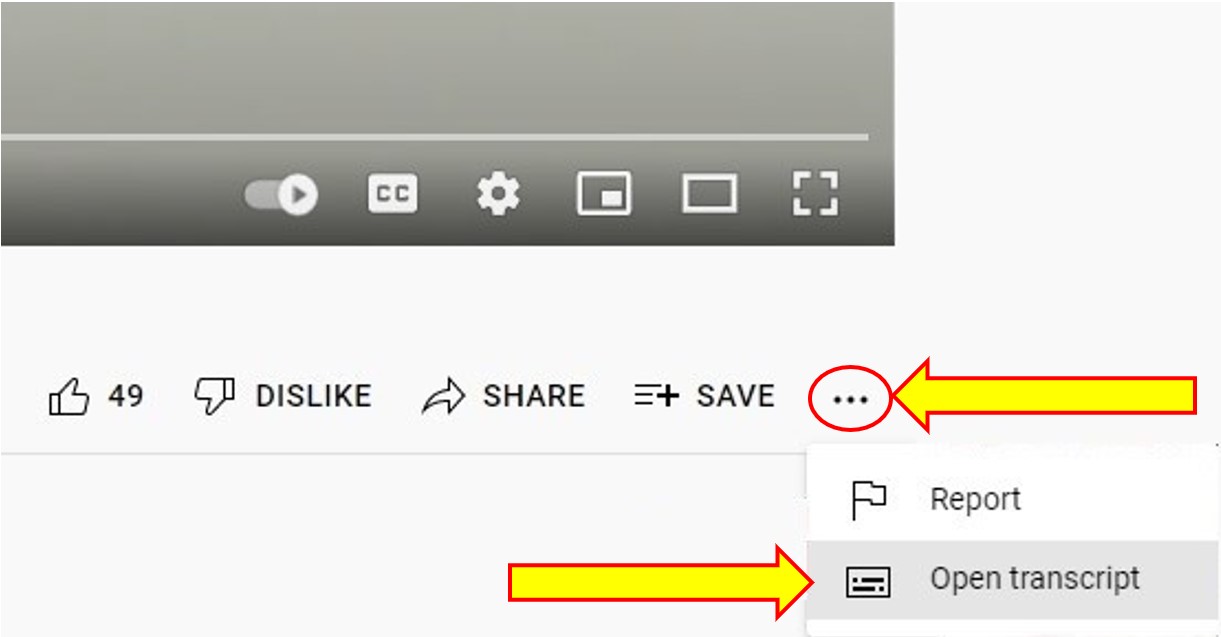
To Access the Video Transcript:
1. Click on “YouTube” on the bottom-right of the video. This will take you directly to the YouTube video.
2. Click on the More Actions icon (represented by three horizontal dots)
3. Click on “Open Transcript”
Please watch the video below to further understand harm reduction in Canada.
The Merits of Harm reduction | Melissa Byers | TEDxGrandePrairie. TEDx Talks. Melissa shares her family’s personal story of addiction and how harm reduction plays a much more significant role to recovery than people realize. She works in the trenches of the current opioid epidemic and her perspective to the issue. Melissa Byers is the Executive Director of Northreach Society, a harm reduction focused organization supporting vulnerable populations in Northern Alberta.(5)
Transcript
To Access the Video Transcript:
1. Click on “YouTube” on the bottom-right of the video. This will take you directly to the YouTube video.
2. Click on the More Actions icon (represented by three horizontal dots)
3. Click on “Open Transcript”
Harm reduction is a philosophy that can humanize the way we see/engage with and support people who live with a substance use disorder and a way we can reduce stigma and help educate the public.
Harm Reduction Services in Canada
Harm reduction strategies can involve any of the following: safer use information, syringe distribution programs, education programs, opiate substitution programs, withdrawal management, safe consumption sites, peer helping and community development. Harm reduction access in Canada depends on the area in which one lives, for example, living in an urban area increases the chances to access harm reduction programs. Research suggests harm reduction services in Canada lack consistency as they are heavily dependent on the provincial governments; organizations lack continuous funding, must participate in a difficult application process for funds, and provinces and territories share different values when it comes to harm reduction (6) (7).
EXPLORE
Please review the interactive Opioid crisis map created by the Government of Canada which indicates harm reduction services focusing on the opioid crisis. Use the map to find locations of opioid-related activities taking place in communities across Canada.
It is not only service providers that are on the front line of harm reduction; it is also critical to acknowledge the work that has been done by the people who use substances. They have advocated for themselves, their peers, and their communities in the face of significant public backlash, threats of incarceration, and inaction on the part of federal, provincial and municipal governments. They have led the harm reduction movement in Canada; they deserve our gratitude: To those who have come before: we are in your debt.
In this section, we will look at some of the more well-known harm reduction programs in Canada. This is by no means a comprehensive list of all harm reduction services across Canada; however, it offers Social workers a snapshot of programs that exist.
Managed Alcohol Programs

Abstinence is not the goal of harm reduction; the goal is to support an individual wherever they may be on the spectrum of substance use. Alcohol is one of the most widely used substances in Canada; alcohol use is on a spectrum. Long term alcohol use has risks, for example average long-term consumption levels as low as one or two drinks per day have been causally linked with significant increases in the risk of at least eight types of cancer and numerous other serious medical conditions including pancreatitis, liver cirrhosis and hypertension (8). Does this mean that everyone who drinks alcohol will develop one of these issues? No, however it increases the risk and when we include the intersectional factors including gender, race, trauma, and add disability, lack of affordable housing, incarceration, and other social determinants of health, we increase the health risks again.
The Canadian Institute on Substance Use Research along with the University of Victoria are currently undertaking a review of harm reduction programs that support individuals with a dependency on alcohol, in particular Managed Alcohol Programs (MAPs). People with severe alcohol dependence who engage in unsafe consumption (amount and consumption of non-beverage alcohol, like hand sanitizer or mouthwash) and a lack of housing are vulnerable to multiple harms (9). Managed Alcohol Programs aim to reduce the harms to individuals who are at risk by providing a safe source of alcohol coupled with services which may include housing, counselling, healthcare, and peer support. “MAPs are harm reduction programs intended to reduce harms of high-risk drinking or severe alcohol use disorder often coupled with ongoing experiences of homelessness or poverty” (10).
There are many different MAP programs in Canada “including community day programs, residential models located in shelters, transitional and permanent housing and hospital-based programs” (11). Every program has different criteria, some address intersectional issues and are gender, race and age specific; nonetheless, all programs have the common goal of preserving dignity and reducing harms of drinking while increasing access to housing, health services, and cultural connections. MAPs have become an important part of harm reduction in Canada.
Heroin Assisted Treatment (HAT)

Opiate use disorders may be managed by heroin assisted therapy (HAT). The first HAT in Canada began in 2005, North America Opiate Medication Initiative (NAOMI) which ran simultaneously in Vancouver and Montreal from 2005-2008 (14). Many participants were living in unstable housing and over 90% of participants had been engaged in some criminal activity during their lifetime (15). Participants were given daily doses of prescription opiates and services to support their other health needs, a comprehensive range of psychosocial and primary care services (16). There was also a control group which received Methadone Maintenance Therapy. The results showed a reduction in average spending on substances, a reduction in illicit-drug use or other illegal activities, an improvement in medical and psychiatric status, improvement in employment satisfaction, and family and social relations (17). There was advocacy to continue the trial for compassionate reasons; however, this was denied by the Canadian Government. “After a year of receiving HAT, participants entered a three-month transition when they were offered a range of traditional treatments, including MMT and detox. After the three-month transitional period, no further treatment or supports were offered” (18).
Opiate use in Canada has been called a crisis (19) and in April 2016, a public health emergency was announced in British Columbia. According to the Government of Canada, there were 22,828 apparent opioid toxicity deaths between January 2016 and March 2021. Since the onset of the COVID-19 pandemic, 6,946 apparent opioid toxicity deaths occurred (April 2020 to March 2021), representing an 88% increase from the same period prior to the pandemic (20). The National Harm Reduction Coalition (2021) (21) suggests there are between 75,000-125,000 people in Canada who are injecting substances, which increases risks of HIV/Hepatitis as well as other blood borne illnesses, bacterial infections, abscesses, and vein collapse. There is much information on safe injection use; however, the risks still exist.
People who have an opiate use disorder come from all walks of life. Opiate use disorder is “a chronic relapsing disease and is often accompanied by abuse of other psychoactive drugs, physical and mental health problems, and severe social marginalization”.(22) For some individuals, abstinence is not an option. Though there are programs like methadone maintenance therapy (MMT), as discussed in Chapter 8, these programs are not universally accessible and not universally successful (23).
A network of individuals who had participated in NAOMI gathered in 2011 to discuss their experiences and this work was collected by Dr. Susan Boyd, culminating in the creation of NAOMI Research Survivors: Experiences and Recommendations (24).
The recommendations from NAOMI participants are listed here:
- When experimental substance maintenance programs are over, clients (research subjects), for compassionate reasons should receive the drug they were on as long as they need it.
- An ideal study would provide an umbrella of support and services including
- housing (most important)
- access to medical treatments all under one roof (nurses, doctors, dentists)
- access to welfare workers (who are familiar with the area and the people who live there) and ministry representatives
- access to nutritious food for self and family
- support to move life forward (school, trade, family unification)
- access to lawyers
- education/advocacy skills and access to advocates
- diverse routes of administration available – oral, smoking form, injection. Not all people want to inject their drug.
This project and the subsequent recommendations helped many working in harm reduction gain a deeper understanding of the research process and the ethics of studies on individuals who use substances.
Providence Health in British Columbia continued this work and launched the Study to Assess Longer-term Opioid Medication Effectiveness (SALOME), which concluded in 2016. This was a clinical trial that tested alternative treatments, specifically prescription opiates, for people with chronic opiate use disorders who were not benefitting from currently known treatments (25). From the success of participants during both the NAOMI and SALOME studies, the courts decided that those who were continuing to benefit from HAT could continue receiving their treatment, though the research was concluded in 2016 (26) (27). There is no current HAT program in Canada.
Syringe Distribution Programs (SDP)
Syringe distribution programs offer clean syringes, alcohol swabs, cookers, water, cottons, all the materials one would need to inject more safely. They also provide safer injection information including safer injection places on the body, vein care, and when to get help. They provide condoms and safer sex information to reduce risks of sexually transmitted infections. They provide a safe space to build relationships, and for those who want to move towards a reduction in use or abstinence, staff at SDP can make referrals to various treatment options. Being a first point of contact has a tremendous amount of responsibility; Social Service workers should have a good understanding of services in their community.

In Vancouver, the epicentre of the HIV crisis in the 1990’s, individuals and agencies were advocating for the development of safer injection. Syringe distribution programs (SDP) began to reduce the spread of blood borne illnesses, including HIV, and since 2018 the Canadian Government has endorsed syringe distribution programs as an effective harm reduction strategy through the pillars of the Canadian Drug and Substances Strategy. Research continues to support the benefit of SDP including a reduction in HIV transmission (28). Syringe distribution is more than just reduction of HIV; through providing a clean needle, it may be the first point of access to a non-judgmental health service for an individual.
Supervised Injection Sites (SIS)

Internationally more than 65 Safe Injection Sites (SIS) have been opened as part of harm reduction strategies associated with substance use (29). Also known as safe consumption sites (SCS), these facilities have been an important part of the harm reduction landscape, particularly in Western Canada since the advent of the HIV crisis and most recently the ongoing public health crisis of opioid overdoses and death (30). SIS are places where people can more safely inject substances using clean equipment under the supervision of medically trained personnel which reduces the risk of overdose and blood borne illnesses. It also allows individuals who may not have had any positive connection to healthcare or other support services to build relationships if they choose.
Most SIS have expanded their mandate to include various forms of consumption. What if substance use is hidden? In rural areas substance use is not always seen in public, which may challenge communities to acknowledge the substance use of its residents.
A common question is whether the site provides the substances. The answer is a resounding no, the substances are not provided by anyone at the facility but are brought there by the individuals who use the service. Most SIS are located in areas where there is a high prevalence of substance abuse and researchers suggest SIS should be developed in areas where injection use and overdose are common (31). The SIS workers help to create a safer space for individuals to use their substance, providing safe equipment, referrals to support services, and in the case of an overdose, medically trained staff to treat the overdose. Many SIS provide “peer assistance.”
Peer assistance refers to one person providing assistance to another in the course of preparing and consuming drugs. Those requiring peer assistance often include women, people with disabilities or illness, and other vulnerable populations. Friends or other clients may help assist, but employees of a supervised consumption site do not directly administer the drugs. (32)
Beyond the services provided regarding preventing overdose and illness, people who use substances are at risk when using in a public area; these risks include being caught by police, being physically or sexually assaulted, or robbed (33). Having a safe place to go reduces those risks. One of the ways SIS are helping to reduce the risk of accidental overdose is using testing kits. People can bring in their substance, have it tested, get information on what is in their substance, which helps them make a more-informed decision about what they use (34). This is a necessity in Canada when substances are bought and sold in the black market. Without regulation, there is risk when you purchase a substance. SIS provide testing kits to prevent overdose and illness.
InSite, a service of PHS Community Services Society, a large non-profit organization in British Columbia, is one of the best known SIS facilities in Canada. InSite was the first safer injection site in Canada. Since its inception, InSite has provided 6,440 overdose interventions without any deaths (35). InSite has also expanded their services to provide safer consumption, which includes more than just injection but the safer consumption of substances that can be taken by other routes of administration, for example, inhalation. InSite has also developed OnSite, a withdrawal management and recovery program.
Please watch the video below and take a virtual tour of InSite.
Inside Insite. NFB (The National Film Board (NFB) is Canada’s public film producer and distributor). To combat Canada’s increasing number of drug overdoses, the federal government introduced legislation that makes it easier to open supervised drug-injection sites. Watch this 360° video to discover more about these life-saving facilities, and step into Canada’s first — and the world’s busiest — supervised drug-injection site. (36)
Transcript
To Access the Video Transcript:
1. Click on “YouTube” on the bottom-right of the video. This will take you directly to the YouTube video.
2. Click on the More Actions icon (represented by three horizontal dots)
3. Click on “Open Transcript”
Overdose Prevention Sites (OPS)
What is the difference between a supervised consumption/supervised injection site and an overdose prevention site (OPS)?
An overdose prevention is less formalized than SCS/SIS. Anecdotal evidence suggests OPS are lower barrier than supervised consumption/supervised injection site and offer the expertise and direct experience of experiential peer workers, filling a much needed service in the tapestry of harm reduction.
Internationally more than 65 Safe Injection Sites (SIS) have been opened as part of harm reduction strategies associated with substance use.(37) Also known as safe consumption sites (SCS), these facilities have been an important part of the harm reduction landscape, particularly in Western Canada since the advent of the HIV crisis and most recently the ongoing public health crisis of opioid overdoses and death(38). SIS are places where people can more safely inject substances using clean equipment under the supervision of medically trained personnel which reduces the risk of overdose and blood borne illnesses. It also allows individuals who may not have had any positive connection to healthcare or other support services to build relationships if they choose. Most SIS have expanded their mandate to include various forms of consumption. What if substance use is hidden? In rural areas substance use is not always seen in public, which may challenge communities to acknowledge the substance use of its residents.
They are generally staffed by peers and harm reduction workers (39). OPS are not required to have health care professionals on staff and are considered “pop-up” as they are a mobile response to overdose prevention.
At the South Riverdale Health Centre in Toronto (40) in Toronto they have a SOS (Safer Opiate Supply) Program. They are one of 4 sites in Toronto that offer the SOS program. The goal is transition people from using toxic and contaminated street opioids and using pharmaceutical grade opioids.
The program is run by 2 Nurse Practitioners, a Community Health Worker, a Program Manager and a Registered Nurse.
All programs are funded by Health Canada’s Substance Use and Addictions Program (SUAP) (41). Referrals for potential clients are received through community partner agencies such as Moss Park OPS, Fred Victor, etc. Self-referrals are not accepted at this time
Naloxone
During the first year of the pandemic, there was a 95% increase in apparent opioid toxicity deaths (April 2020 – March 2021, 7,224 deaths), compared to the year before (April 2019 – March 2020, 3,711 deaths). Since then, deaths have remained high. (42)

In Canada, two types of take-home kits are available (43) :
- Naloxone nasal spray is sprayed directly into the nose, where it is absorbed. It starts to take effect in 2 to 3 minutes. Learn how to give naloxone spray (video).
- Naloxone injectable is injected into any muscle in the body, such as the arm or thigh. It starts to take effect in 2 to 3 minutes. Learn how to give a naloxone injection (video).
One way to prevent overdose deaths, as part of a comprehensive harm reduction strategy, is to ensure individuals and communities have access to naloxone, an opioid antagonist to an opioid overdose.
Where to get naloxone in your province or territory (43)
Take-home naloxone kits are available at most pharmacies. A prescription is not needed. Ask the pharmacist.
Some provinces offer free take-home naloxone kits. Consult your province to see where these kits are available.
-
- Alberta
- British Columbia
- Manitoba
- New Brunswick – Naloxone kits are available at pharmacies.
- Newfoundland and Labrador
- Northwest Territories
- Nova Scotia
- Nunavut
- Ontario
- Prince Edward Island
- Quebec
- Saskatchewan
- Yukon
Food For Thought
- Why would some pilot projects on substance use disorders do not get funded?
- What is the role of media in sharing information?
- What is the role of activism/advocacy?
Naloxone kits are just one component; helping individuals understand the risks of using a substance alone is another arm of naloxone.
Please watch the following video on never using alone.
How to Spot Someone so They Never Use Alone. By Canadian Association of People Who Use Drugs (CAPUD). This is the launch of an educational animation about spotting – an overdose prevention method done by phone or video call. This new resource from CAPUD is available in both official languages and provides an step by step guide about spotting. (44)
Transcript
To Access the Video Transcript:
1. Click on “YouTube” on the bottom-right of the video. This will take you directly to the YouTube video.
2. Click on the More Actions icon (represented by three horizontal dots)
3. Click on “Open Transcript”
There are many forms of harm reduction and many harm reduction programs in Canada. Harm reduction is an important pillar in healthcare for people who use substances.
For information on all Harm Reduction Programs in Toronto, visit a student run organization called Harm Reduction TO. They also have great ways for students who are looking to become involved in changing the approach to substance use by “ending the war on drugs.”
Attribution:
“Exploring Substance Use in Canada” by Julie Crouse is licensed under CC BY-NC-SA 4.0
References
- International Harm Reduction Association. (2021). What is harm reduction. https://www.hri.global/what-is-harm-reduction
- Hyshka, E., Anderson-Baron, J., Karekezi, K., Belle-Isle L., Elliott, R., Pauly, B., Strike, C., Asbridge, M., Dell, C., McBride, K., Hathaway, A., & Wild, T. C. (2017). Harm reduction in name, but not substance: A comparative analysis of current Canadian provincial and territorial policy frameworks. Harm Reduction Journal, 14(1), 50. https://doi.org/10.1186/s12954-017-0177-7
- Harm Reduction. (n.d.). https://ontario.cmha.ca/harm-reduction/#:~:text=Harm%20Reduction%20is%20an%20evidence,substances%20from%20abstaining%20or%20stopping.
- Toronto Harm Reduction Alliance. (2020, June 3). #SupplyOrWeDie – Toronto Harm Reduction Alliance [Video]. YouTube. https://www.youtube.com/watch?v=leT5IQVWk24
- TEDx Talks. (2019, November 6). The Merits of Harm reduction | Melissa Byers | TEDxGrandePrairie [Video]. YouTube. https://www.youtube.com/watch?v=qU_MWjIUFmE
- Hyshka, E., Anderson-Baron, J., Karekezi, K., Belle-Isle L., Elliott, R., Pauly, B., Strike, C., Asbridge, M., Dell, C., McBride, K., Hathaway, A., & Wild, T. C. (2017). Harm reduction in name, but not substance: a comparative analysis of current Canadian provincial and territorial policy frameworks. Harm Reduction Journal, 14(1), 50. https://doi.org/10.1186/s12954-017-0177-7
- Cavalieri, W., & Riley D (2012). Harm reduction in Canada: The many faces of regression. In Pates & D. Riley (Eds.), Harm reduction in substance use and high risk behaviour: international policy and practice (pp. 392–394). Wiley-Blackwell.
- Butt, P., Beirness, D., Cesa, F., Gliksman, L., Paradis, C., & Stockwell, T. (2011). Alcohol and health in Canada: A summary of evidence and guidelines for low-risk drinking. Canadian Centre on Substance Abuse. https://www.uvic.ca/research/centres/cisur/assets/docs/report-alcohol-and-health-in-canada.pdf
- Pauly B. B., Reist, D., Belle-Isle, L., & Schactman, C. (2013). Housing and harm reduction: What is the role of harm reduction in addressing homelessness? International Journal on Drug Policy, 24(4), 284–290.
- Canadian Institute for Substance Use Research. (n.d.). Scale up of managed alcohol programs. Bulletin #20. 1-4. https://www.uvic.ca/research/centres/cisur/assets/docs/bulletin-20-scale-up-of-maps.pdf
- Canadian Institute for Substance Use Research. (n.d.). Scale up of managed alcohol programs. Bulletin #20. 1-4. https://www.uvic.ca/research/centres/cisur/assets/docs/bulletin-20-scale-up-of-maps.pdf
- Canadian Institute for Substance Use Research. (2021). Overview of Managed Alcohol Program (MAP) sites in Canada (and beyond). https://www.uvic.ca/research/centres/cisur/assets/docs/resource-overview-of-MAP-sites-in-Canada.pdf
- CBC. (2016). The Fifth Estate: The Pour. https://www.cbc.ca/player/play/849395779835
- Oviedo-Joekes, E., Nosyk, B., Brissette, S., Chettiar, J., Schneeberger, P., Marsh, D. C., Krausz, M., Anis, A., & Schechter, M. T. (2008). The North American Opiate Medication Initiative (NAOMI): Profile of participants in North America’s first trial of heroin-assisted treatment. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 85(6), 812–825. https://doi.org/10.1007/s11524-008-9312-9
- Oviedo-Joekes, E., Nosyk, B., Brissette, S., Chettiar, J., Schneeberger, P., Marsh, D. C., Krausz, M., Anis, A., & Schechter, M. T. (2008). The North American Opiate Medication Initiative (NAOMI): Profile of participants in North America’s first trial of heroin-assisted treatment. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 85(6), 812–825. https://doi.org/10.1007/s11524-008-9312-9
- Ibid
- Berridge, V. (2009). Heroin prescription and history. The New England Journal of Medicine, 361, 820-821. https://psycnet.apa.org/doi/10.1056/NEJMe0904243
- The NAOMI Patients Association & Boyd, S. (2012). NAOMI research survivors; experiences and recommendations (p. 20). https://drugpolicy.ca/wp-content/uploads/2012/03/NPAreportMarch5-12.pdf
- Government of Canada. (2021, Sept. 22). Opioid- and stimulant-related harms in Canada. https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/
- Ibid
- The National Harm Reduction Coalition. (2021). Priniciples of harm reduction. https://harmreduction.org
- Van den Brink, W., & Haasen, C. (2006). Evidenced-based treatment of opioid-dependent patients. Canadian Journal of Psychiatry, 51, 635–646. https://doi.org/10.1177/070674370605101003
- Goldstein, M. F., Deren, S., Kang, S. Y., Des Jarlais, D. C., & Magura, S. (2002). Evaluation of an alternative program for MMTP drop-outs: Impact on treatment re-entry. Drug Alcohol Dependence, 66, 181–187. https://doi.org/10.1016/S0376-8716(01)00199-5
- The NAOMI Patients Association & Boyd, S. (2012). NAOMI research survivors; experiences and recommendations. https://drugpolicy.ca/wp-content/uploads/2012/03/NPAreportMarch5-12.pdf
- Providence Health Care. 2016. SALOME. https://www.providencehealthcare.org/salome/about-us.html
- Canadian Drug Policy. (2021). Heroin assisted treatment. https://drugpolicy.ca/our-work/issues/heroin-assisted-treatment/
- Providence Health Care. 2016. SALOME. https://www.providencehealthcare.org/salome/about-us.html
- Canadian Agency for Drugs and Technology in Health. (2015). Needle exchange programs in a community setting: A review of the clinical and cost effectiveness. https://cadth.ca/sites/default/files/pdf/htis/2017/RC0705%20Needle%20Exchange%20in%20Community%20Final.pdf
- Marshall, B. D., Milloy, M. J., Wood, E., Montaner, J. S., & Kerr, T. (2011). Reduction in overdose mortality after the opening of North America’s first medically supervised safer injecting facility: a retrospective population-based study. The Lancet, 377(9775), 1429-1437. https://doi.org/10.1016/S0140-6736(10)62353-7
- Government of Canada. (2021, Sept. 22). Opioid- and stimulant-related harms in Canada. https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/
- Marshall, B. D., Milloy, M. J., Wood, E., Montaner, J. S., & Kerr, T. (2011). Reduction in overdose mortality after the opening of North America’s first medically supervised safer injecting facility: a retrospective population-based study. The Lancet, 377(9775), 1429-1437. https://doi.org/10.1016/S0140-6736(10)62353-7
- Government of Canada. (2021, Nov. 11). Supervised consumption sites: Status of applications.https://www.canada.ca/en/health-canada/services/substance-use/supervised-consumption-sites/status-application.html
- Green, T. C., Hankins, C. A., Palmer, D., Boivin, J. F., & Platt, R. (2004). My place, your place or a safer place: The intention among Montreal injecting drug users to use SIF. Canadian Journal of Public Health, 95(2),110-114. https://www.jstor.org/stable/41994109
- Maghsoudi, N., Tanguay, J., Scarfone, K., Rammohan, I., Ziegler, C., Werb, D., & Scheim, A. (2021). The implementation of drug checking services for people who use drugs: A systematic review. Qeios. https://doi.org/10.32388/TXE86U
- Vancouver Coastal Health. (2020). Supervised consumption sites. http://www.vch.ca/public-health/harm-reduction/supervised-consumption-sites
- National Film Board of Canada (2017, May 26). Inside Insite. [Video]. Youtube. https://www.youtube.com/watch?v=7gIyBMt2BEk
- Marshall, B. D., Milloy, M. J., Wood, E., Montaner, J. S., & Kerr, T. (2011). Reduction in overdose mortality after the opening of North America’s first medically supervised safer injecting facility: a retrospective population-based study. The Lancet, 377(9775), 1429-1437. https://doi.org/10.1016/S0140-6736(10)62353-7
- Government of Canada. (2021, Nov. 11). Supervised consumption sites: Status of applications. https://www.canada.ca/en/health-canada/services/substance-use/supervised-consumption-sites/status-application.html
- Pauly, B., Wallace, B., Pagan, F., Phillips, J., Wilson, M., Hobbs, H., & Connolly, J. (2020). Impact of overdose prevention sites during a public health emergency in Victoria, Canada. PLoS One, 15(5). https://doi.org/10.1371/journal.pone.0229208
- Safer Opiate Supply (SOS) – SRCHC. (n.d.). https://www.srchc.ca/programs/community-health/safer-opiate-supply-sos/
- Health Canada. (2022b, April 21). Health Canada’s Substance Use and Addictions Program. Canada.ca. https://www.canada.ca/en/health-canada/services/substance-use/canadian-drugs-substances-strategy/funding/substance-use-addictions-program.html
- Opioid- and stimulant-related harms — Canada.ca. (2023b, March 27). https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants
- Health Canada. (2023c, March 14). Naloxone. Canada.ca. https://www.canada.ca/en/health-canada/services/opioids/naloxone.html
- Canadian Association of People who Use Drugs. (2021). How to spot someone so they never use alone. [Video]. Youtube. https://www.youtube.com/watch?time_continue=3&v=KbUwb-pszW4&feature=emb_logo
- Harm Reduction TO. (n.d.). Harm Reduction TO. https://harmreductionto.ca/
